IgA 신 병증(IgA 콩팥병증/IgA 신장병증/베르게르 병) IgA Nephropathy(IgA nephritis/Berger’s disease)
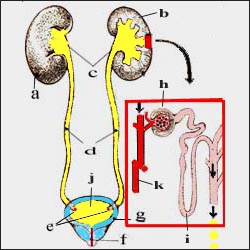
그림 1-1. 신장, 비뇨계 구조
a-우 신장, b-좌 신장, c-신우, d-요관, e-요관구, f-요도, g-방광, h-사구체, i-헨레계제, j-소변, k-혈관. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
-
이병을 영어로 IgA nephritis, IgAN, Berger’s disease, Berger’s syndrome 또는 synpharyngitic glomerulonephritis이라고 부르기도 한다. glomerulonephritis(사구체 염)의 일종이다.
-
신장 조직에 아이지에이(IgA) 항체가 침착되어 이 병이 생긴다.
-
육안적 혈뇨 또는 현미경적 혈뇨가 나타나고, 때로는 단백뇨나 고혈압 등이 생길 수 있다.
-
이 병은 만성 사구체 신염의 일종으로서, 베르게르 병이라고도 부른다.
-
이 병은 과거 10년 동안에 새로운 병으로 등장했다.
-
미국·일본 등 세계 각국에서 발병된다.
-
여성보다 남성에게 이 병이 더 잘 생긴다.
-
바이러스 상기도염을 앓은 후 1~3일에 발생되는 것이 보통이다.
-
육안으로 볼 수 있는 혈뇨가 나타날 수 있다.
-
혈뇨는 발병 후 며칠 동안 지속될 수 있으며, 자연히 없어지고 재발되는 것이 보통이다.
-
A군 연쇄상구균 감염 후 생기는 급성 사구체 신염은 A군 베타 용혈성 연쇄상구균성 피부염이나 인두염을 앓은 후 약 1~3주에 발병되는 것이 보통이지만, 아이지에이(IgA) 신 병증은 바이러스 상기도염을 앓은 후 1~3일에 발병된다.
-
IgA 신 병증을 앓는 아이들의 일부에게서 고혈압, 신증후군, 진행성 사구체 신염 신부전증 등이 생길 수 있다.
-
때로는 이 병이 있어도 아무 증상 없이 혈뇨만 나타날 수 있고, 혈뇨와 단백뇨가 같이 있을 때도 있다.
IgA 신 병증(IgA 콩팥병증/IgA 신장병증/베르게르 병)의 진단
-
병력, 증상 징후, 신체검사, 소변검사, 신장 생체 조직 검사와 임상검사 등으로 진단한다.
-
A군 연쇄상구균 감염 후 생기는 급성 사구체 신염, 전신 홍반성 낭창 급성 사구체 신염, 헤노흐–쇤라인 자반증, 급성 사구체 신염,특발성 신중후군 등과 감별진단해야 한다.
IgA 신 병증(IgA 콩팥병증/IgA 신장병증/베르게르 병)의 치료
-
-
특효약은 없다.
-
임상 검사, 특히 소변검사, 혈압 측정 등을 주기적으로 해서 이 병의 진행 정도를 알아보고 그때그때의 증상 징후에 따라 치료한다.
-
코르티코스테로이드제, Cyclosporine, Phenytoin, 또는 생선 오일 등으로 치료할 수 있다. 그러나 치료 효과는 확실치 않다.
-
IgA nephropathy (IgA nephritis/Berger’s disease) IgA 신 병증(IgA 콩팥병증/IgA 신장병증/베르게르 병)
Figure 1-1. Structure of the kidneys and urinary system a-right kidney, b-left kidney, c-renal right, d-ureter, e-ureter, f-urethra, g-bladder, h-glomera, i-Henre system, j-urine, k-vessel. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
• This disease is sometimes called IgA nephritis, IgAN, Berger’s disease, Berger’s syndrome or synpharyngitic glomerulonephritis in English. It is a type of glomerulonephritis. • This disease is caused by deposits of IgA antibodies in kidney tissue.
• Gross hematuria or microscopic hematuria may appear, sometimes proteinuria or high blood pressure.
• This disease is a type of chronic glomerulonephritis, also called Berger’s disease.
• This disease has emerged as a new disease in the past 10 years.
• Outbreaks occur in countries around the world including the United States and Japan.
• Men are more likely to develop this disease than women.
• It usually occurs 1 to 3 days after suffering from viral upper respiratory tract infection.
• Visible hematuria may occur.
• Hematuria can last for several days after onset, and it usually goes away and recurs spontaneously.
• Acute glomerulonephritis after group A streptococcal infection usually develops about 1 to 3 weeks after suffering from group A beta hemolytic streptococcal dermatitis or pharyngitis. It develops 1 to 3 days after.
• Some children with IgA nephropathy may develop high blood pressure, nephrotic syndrome, progressive glomerulonephritis and kidney failure.
• Sometimes, even with this disease, only hematuria can appear without any symptoms, and hematuria and proteinuria are also present.
Diagnosis of IgA nephropathy (IgA nephropathy/IgA nephropathy/Berger’s disease)
• Diagnosis is based on medical history, symptom signs, physical examination, urine examination, kidney biopsy and clinical examination.
• Acute glomerulonephritis after group A streptococcal infection, systemic lupus erythematosus, acute glomerulonephritis, Henoch-Schoen’s purpura, acute glomerulonephritis, and idiopathic cautious syndrome should be differentially diagnosed.
Treatment of IgA nephropathy (IgA nephropathy/IgA nephropathy/Berger’s disease)
• o There is no special drug.
o Clinical tests, especially urine tests, blood pressure measurements, etc. are performed periodically to check the progression of the disease and treat it according to the symptoms and symptoms at that time.
o It can be treated with corticosteroids, Cyclosporine, Phenytoin, or fish oil. However, the effectiveness of the treatment is uncertain.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com 제7권 소아청소년 감염병
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”