A군 베타 용혈성 연쇄상구균 인두 편도염(A군 연구균 인두 편도염) Group A β hemolytic streptococcal pharyngotonsillitis(Group A streptococcal pharyngotonsillitis)
| A군 베타 용혈성 연쇄상구균 인두 편도염의 원인 |
- A군 베타 용혈성 연쇄상구균이란 박테리아가 인두에만 감염 되어 생긴 급성 인두염을 A군 베타 용혈성 연쇄상구균 인두염이라고 한다.
- 또 편도에만 감염 되어 편도염만 생겼을 때는 A군 베타 용혈성 연쇄상구균 편도염이라고 한다. 급성 편도염에서 이미 많이 설명했지만 여기서는 더 구체적으로 설명한다.
- 또 그 균의 감염으로 인두와 편도에 동시 감염 되어 인두염과 편도염이 동시 생겼을 때는 A군 베타 용혈성 연쇄상구균 인두편도염이라고 한다.
- 이론적으로 이렇지만, 실제로는 인두와 편도는 협소한 인두강 속에서 서로 인접되어 있기 때문에 감염성이 아주 강한 A군 베타 용혈성 연쇄상구균이 인두에만 감염되지 않고 또 편도에만 감염되지 않고 인두와 편도에 동시 함께 감염되어 A군 베타 용혈성 연쇄상구균 인두염과 A군 베타 용혈성 연쇄상구균 편도염이 동시 함께 생기는 것이 일반적이다.
- 다시 설명하면, A군 베타 용혈성 연쇄상구균이 목안 즉 인두강 점막층에 감염 될 때는 인두에만 또는 편도에만 따로따로 감염 될 수 없다.
- 그래서 인두와 편도에 동시에 감염 되어 그 두 부위에 감염병을 동시 일으켜 A군 베타 용혈성 연쇄상구균 인두 편도염(Group A β hemolytic streptococcal pharyngotonsillitis)이 동시 생기는 것이 보통이다. 이때는 박테리아 인두 편도염(Viral pharyngotonsillitis)이라고 한다.
- 또 A군 베타 용혈성 연쇄상구균 이외 다른 종류의 박테리아나 아데노바이러스 등 바이러스 감염으로 인두강 내 감염병이 생길 때도 편도에만, 또는 인두에만 감염병이 따로따로 생기지 않고 편도와 인두 두 부위에 동시 감염병이 생기는 것이 보통이다.
- 그런데 A군 베타 용혈성 연쇄상구균 감염으로 생긴 인두편도염을 A군 베타 용혈성 연쇄상구균 인두염, A군 베타 용혈성 연쇄상구균 인두편도염, 또는 A군 베타 용혈성 연쇄상구균 편도염이라는 병명을 임상에서 다른 병명과 같이 부르기도 한다.
- 또 다른 병명을 붙여 다루는 때도 많기 때문에 의사도 환자도 부모도 혼동할 때가 많다. 여기서 이 세 가지 병명은 사실은 의학적으로 거의 같은 병명이다.
| A군 베타 용혈성 연쇄상구균 인두 편도염의 증상 징후 |

사진 54. A군 베타 용혈성 연쇄상구균 인두염과 편도염으로 편도가 붓고 빨갛다.
출처-Copyrightⓒ 2011 John Sangwon Lee,MD.FAAP

사진 55.A군 베타 용혈성 연쇄상구균 인두염과 편도염으로 편도가 붓고 연구개(입천장)가 빨갛다. 여기서 분 편도염은 보이지 않는다. 하얀 곱이 혓바닥에 끼어 있다.
출처-Copyrightⓒ 2011 John Sangwon Lee,MD.FAAP

사진 56.심한 A군 베타 용혈성 연쇄상구균 인두염과 편도염.
편도가 붓고 빨갛고 흰 곱이 꼈다. 목젖염으로 목젖이 붉고 부어 있다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP

사진 57.심한 A군 베타 용혈성 연쇄상구균 인두염과 편도염. 붓고 빨간 편도에 곱이 끼었다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 58. A군 베타 용혈성 연쇄상구균 편도염과 인두염
편도염으로 양쪽 편도가 상당히 비대 됐다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP

사진 59. A군 베타 용혈성 연쇄상구균 편도염과 인두염으로 양쪽 편도가 조금 부었다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP

사진 60. A군 베타 용혈성 연쇄상구균 감염으로 편도염도 생길 수 있고 성홍열도 생길 수 있다. 성홍열의 증상 징후로 혓바닥에 하얀 백태가 낄 수 있고 그 다음, 그 혀가 빨간 딸기 색과 비슷한 빨간 혓바닥 색으로 일시적으로 변할 수 있다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP

사진 61.A군 베타 용혈성 연쇄상구균 감염이 편도에 생겼고 성홍열도 생길 수 있다.
이 때 성홍열의 증상 징후로 처음에는, 혓바닥에 하얀 백태가 낄 수 있고 그 다음에는 그 혀가 빨간 딸기 색과 비슷한 혓바닥 색으로 변할 수 있다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP

사진 62. A군 베타 용혈성 연쇄상구균 감염이 편도와 인두에 생길 수 있고 성홍열도 생길 수 있다. 성홍열로 손바닥의 피부의 각질층이 얇게 벗겨졌다.
출처-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
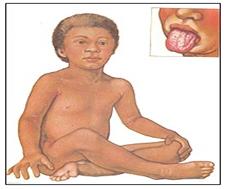
그림 63. A군 베타 용혈성 연쇄상구균 감염이 편도에 생기고 성홍열도 생길 수 있다. 성홍열을 앓을 때 사포와 비슷하게 도돌도돌한 피부 발진이 생길 수 있다. 피부 발진의 색은 붉은 것이 보통이다. 출처; Used with permission from Health information service Merk Sharp & Dome, West Point, PA
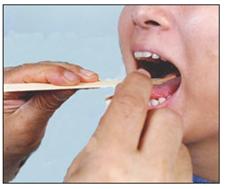
사진 64. A군 베타 용혈성 연쇄상구균 세균 배양 검사를 하기 위해 또는 항체 항원 응급 반응 검사를 하기 위해 인두 점막에서 점액을 채취한다.
출처-Copyright ⓒ 2012 John Sangwon Lee, MD. FAAP
- A군 베타 용혈성 연쇄상구균 인두 편도염의 증상 징후는 환아 나이, 병의 진행 경과, 합병증의 유무 등에 따라 다르다.
A군 베타 용혈성 연쇄상구균 인두 편도염의 전형적 증상 징후
- 편도가 붉어지고, 붓고, 곪으면서 커지며, 목안이 몹시 아프다.
- 미열 내지 고열이 나고,
- 두통, 복통, 구토 등의 증상 징후가 있으면서 팔다리와 전신이 아프다.
- 환아가 독성상태에 빠져 있는 것이 보통이다.
- 전등불로 인두와 편도를 비춰 육안으로 들여다보면 편도, 인두와 연구개 부위가 빨개진 것을 볼 수 있다.
- 이 병이 발병된 후 2~3일이 되었을 때 편도에 하얀 고름과 곱이 끼고, 편도가 크게 부어 있는 것을 쉽게 볼 수 있다.
- 턱 바로 밑 목 림프절이 부을 수 있고, 그것을 손으로 만지면 조금 아플 수 있다.
- 이 병은 초기에 적절한 항생제로 적절히 치료해 주지 않으면 점점 더 악화되는 것이 보통이다.
- 더 심해지면 인두가 점점 더 아프고, 침과 음식물도 삼키기가 어려울 정도로 인두통이 더 심하게 된다.
- 어떤 때는 환아가 몹시 아파 보이고 놀기를 싫어하며 잠만 자려고 한다.
- 독성 상태에 빠지기도 한다.
- 식욕이 떨어져서 음식물을 잘 먹지 않으며 잠을 비정상적으로 많이 자거나 잘 자지 못한다.
- A군 베타 용혈성 연쇄상구균의 여러 균종 중 발적 독소를 생성하는 균종의 감염으로 인두편도염이 생기고 그와 동시에 성홍열도 나타날 수 있다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제7권 소아청소년 감염병-성홍열 참조
- A군 베타 용혈성 연쇄상구균 인두편도염이 있으면서 피부에 발진이 생기고, 혓바닥에 흰 곱이 초기에 끼었다가 그 다음은 빨간 딸기 색과 비슷하게 혓바닥이 빨갛게 변하는 증상 징후가 생긴다. 이럴 때의 급성 인두편도염을 A군 베타 용혈성 연쇄상구균 인두편도염이라는 병명을 붙이는 대신 성홍열이란 병명을 부쳐 진단한다.
A군 베타 용혈성 연쇄상구균 감염병의 합병증
A군 베타 용혈성 연쇄상구균 감염으로 인한 인두 편도염을 적절히 치료하지 않으면 생명이 위험할 수 있다.그리고 다음과 같은 합병증이 생길 수 있다
- 급성 사구체신염,
- 류마티스 열,[부모도 반의사가 되어야 한다-소아가정간호백과]-제11권 소아청소년 심장 혈관계 질환-류마티스 열 참조)
- 류마티스 심장염 (Rheumatic carditis,)
- 패혈증,
- 중이염,
- 축농증,
- 골수염,
- 관절염
- 그 외 여러 가지 합병증이 생길 수 있다.
A군 베타 용혈성 연쇄상구균 인두 편도염의 진단
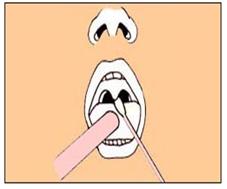
그림 65 .A군 베타 용혈성 연쇄상구균을 세균배양하거나 A군 베타 용혈성 연쇄상구균 항원 항체 응집반응 검사를 하기 위해 인두나 편도의 점막에서 점액을 면봉으로 채취한다.
출처-Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
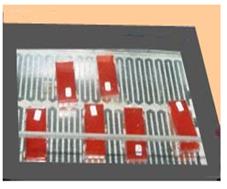
사진 66.인두 점막층에서 채취한 점액을 혈액 우무 세균배양지에 묻힌 후 그 세균 배양지를 세균배양을 하는 인큐베이터에 넣고 24시간 동안 세균배양을 한다. 이런 검사는 동네병원에서도 쉽게 할 수 있다. 진단상 정확성은 좋은 반면 검사비가 많이 든다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
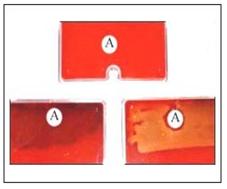
사진 67.세균배양 인큐베이터 속에 넣기 바로 전 피검 물 점액을 묻힌 혈액 우무 세균배양지(상)
A군 베타 용혈성 연쇄상구균이 아닌 잡균이 자란 세균배양지(하좌)
A군 베타 용혈성 연쇄상구균이 아닌 다른 종류의 연구균이 자란 혈액 우무 세균 배양지(하우)
A는 택소이다. 택소는 많은 종류의 연쇄상구균의 군종들 중 A군만 배양 검출하는 데 쓰는 항생제 디스크이다.
A 택소의 바로 주위에는 A군 연구균이 자라지 못해 원래 혈핵 우무 세균배양지의 색과 거의 비슷한 색으로 보인다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
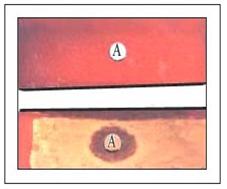
사진 68.세균배양 인큐베이터 속에 넣었던 혈액 우무세균 배양지에 A군 베타 용혈성 연쇄상구균은 자라기 않고 잡균만 자랐다(상). A군 베타 용혈성 연쇄상구균만 혈액 우무세균 배양지에 자랐다(하).
A는 택소이다. 택소는 많은 종류의 연쇄상구균의 군종들 중 A군만 배양 검출하는 데 쓰는 항생제 디스크이다.
A 택소의 바로 주위에는 A군 연구균이 자라지 못해 원래 혈액 우무 세균배양지의 색과 거의 비슷한 색으로 보인다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP

사진 70. A군 베타 용혈성 연쇄상구균 항원 항체 응집 반응검사가 양성으로 나타난 것
요즘 새로 나온 BioStar Strep A Ola Max rapid strep test로 항원 항체 응집 반응 검사를 하면 그 검사 결과가 96% 특이성 진단 가치가 있다. 그래서 A군 베타 용혈성 연쇄상구균 배양 검사를 꼭 할 필요가 없고 이 검사만으로 A군 베타 용혈성 연쇄상구균 인두편도염을 진단하기에 충분한 조건이 된다고 한다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
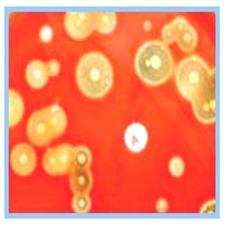
사진71.병원 세균 검사실에서 하는 A군 베타 용혈성 연쇄상구균 배양을 한다.
Copyrightⓒ 2011 John Sangwon Lee,MD., FAAP
- 병력, 증상 징후, 진찰소견 등을 종합하여 이 병이 의심되면 인두 점막층이나 편도 점막층에서 면봉으로 점액을 채취하여 그 피검 물로 A군 베타 용혈성 연쇄상구균 항원 항체 응집 반응 검사를 하면 5-10분 이내에 진단할 수 있다.(사진 69, 70 참조.)
- 또는 면봉에 묻은 점액으로 A군 베타 용혈성 연쇄상구균 세균배양 검사(스트렙토 배양 검사)를 해서 24시간 이내에 확진할 수 있다.
- 앞서 설명한 여러 가지 증상 징후와 인두통이 있으면 바이러스 인두 편도염이 있는지 A군 베타 용혈성 연쇄상구균으로 인해 생긴 박테리아 인두 편도염이 있는지 알아보아야 한다.
|
인두 점막 면봉 채집 피검물 세균 배양 검사에서 수막구균이 배양될 때
|
A군 베타 용혈성 연쇄상구균 인두 편도염의 치료
- 의사의 처방에 따라 A군 베타 용혈성 연쇄상구균 인두 편도염은 페니실린, 에리스로마이신, 또는 세팔로스포린(Cephalosporin)계 항생제 중 한 가지 항생제로 적절히 치료한다.
- 세팔로스포린(Cephalosporins)계 항생제에는 Cephalexin, Cephadroxil, Cefuroxime, Cefpodoxime, Cefprozil, Cefixime, Ceftibuten, Cefdinir 등 여러 종류가 있다.
- 그 중 한 가지를 선택해 치료하면 페니실린으로 치료하는 것보다 더 효과가 있다고 한다([부모도 반의사가 되어야 한다-소아가정간호백과]-제7권 소아청소년 감염병-표 1-10 참조).
- 바이러스 감염으로 생긴 인두 편도염을 항생제로 치료해 주어도 이 병에 아무런 치료효력이 없을 뿐만 아니라 그런 항생제 치료에 의해서 부작용이 생길 수 있다.
- 그밖에 다른 여러 가지 이유로 항생제로 함부로 치료해서도 안 된다.
- A군 베타 용혈성 연쇄상구균 감염으로 인한 인두편도염을 페니실린이나 에리스로마이신 등 항생제로 치료할 때 항생제에 치료효력이 나면 치료시작 한지 1~2일 이내 열이 떨어지고 인두통과 전신이 아픈 증상이 거의 없어지는 것이 보통이다.
- 그러나 처방한 항생제 권장 복용기간 동안 꼭 복용해서 A군 베타 용혈성 연쇄상구균을 박멸시켜 주어야 인두편도염이 재발되지 않는다.
- 항생제의 종류에 따라 치료 기간이 다를 수 있다.
- 열이 나고 인두가 아플 때는 타이레놀이나 모트린(Motrin/Ibuprofen) 등의 해열 진통제로 필요에 따라 대증치료를 한다.
- 열이 내리고 인두가 더 이상 아프지 않을 때까지 육체적 휴식을 취해야 한다.
- 적절한 항생제로 치료를 시작한 지 24시간 이후부터 전반적으로 증상 징후가 호전되고 평상시 건강 상태로 점점 뒤돌아 가면 학교에 보내도 된다.
- 인두에 아무런 약도 바를 필요 없고 인두 편도염을 앓았다고 해서 편도절제 수술치료를 꼭 받을 필요도 없다. 편도 절제 수술 참조.
- A군 베타 용혈성 연쇄상구균은 다른 사람에게 잘 감염된다.
- 그러므로 한 집안 식구들 중 누군가가 목구멍이 아프고 열이 나면서 앓으면 의사의 진단 치료를 곧 받아야 한다.
- A군 베타 용혈성 연쇄상구균 감염을 예방접종할 수 있는 백신은 아직 없다.
- 의사가 처방한 대로 항생제를 일정한 기간 동안 꼭 다 복용해야 한다.
미크롤라이드(마이크로라이드/Microrides) 항박테리아 항생물에 내성이 생기는 A군 베타 용혈성 연쇄상구균
- A군 베타 용혈성 연쇄상구균 감염으로 인한 편도염이나 인두염 등은 페니실린이나 에리스로 마이신 등 항생제 치료로 과거에는 잘 치료됐으나 요즘에는 미 전역에서 A군 베타 용혈성 연쇄상구균이 미크롤라이드 항생물질 치료에 내성이 생겨 A군 베타 용혈성 연쇄상구균 감염으로 인한 편도염이나 인두염 등이 에리스로마이신 등 미크롤라이드 항생물질로 잘 치료되지 않아 문제가 생기고 있다.
미 감염병 학회의 연쇄상 구균 인두염 진단 치료 가이드
Group A streptococcal (GAS) pharyngitis.Guidelines – Updated
- 신속 항원 항체 응집검사로 진단하거나 인두점액 피검물로 연쇄상구군 세균 배양검사로 진단하고
- 소아 청소년 환아에서 신속 항원 항체 응집(반응)검사 결과가 음성으로 나타나면 인두 점액 피검물로 연쇄상구군 세균배양검사를 하여 확진하고
- 성인 환자에서는 신속 항원 항체 응집검사 결과가 음성으로 나타나도 인두 점액 피검물로 연쇄상구군 세균배양검사로 확진하지 않아도 된다.
- 기침, 콧물, 입안 궤양 등의 바이러스 감염의 증상 징후가 있으면 연쇄상구군 세균 검사를 않아도 된다.
- 형제자매가 연쇄상 구균에 의한 감염병이 있지 않으면 3세 이하 영유아들은 연쇄상구군 세균 검사를 하지 않아도 된다.
- 페니실린에 알레르가 없으면 Penicillin 또는 Amoxicillin으로 10일간 치료한다. .
- 페니실린에 알레르기가 있으면 Cephalosporin, Clindamycin, Clarithromycin, 또는 Azithromycin으로 치료한다. 소스 : IDSAInfectious Diseases Society of America Issues Strep Guidelines 2012년 9월
Group A β hemolytic streptococcal pharyngotonsillitis (Group A streptococcal pharyngotonsillitis) A군 베타 용혈성 연쇄상구균 인두 편도염(A군 연구균 인두 편도염)
Causes of group A beta hemolytic streptococcal pharyngeal tonsillitis
• Group A beta hemolytic streptococci is an acute pharyngitis caused by bacterial infection only in the pharynx and is called group A beta hemolytic streptococcal pharyngitis.
• In addition, when only tonsillitis occurs due to infection only in the tonsils, it is called group A beta hemolytic streptococcal tonsillitis. We have already described a lot in acute tonsillitis, but we will explain it more specifically here.
• In addition, when pharyngitis and tonsillitis occur simultaneously due to infection of the pharynx and tonsils due to infection of the fungus, it is called group A beta hemolytic streptococcal pharyngeal tonsillitis.
• This is theoretically, but in reality, the pharynx and tonsils are adjacent to each other in the narrow pharyngeal cavity. Therefore, group A beta hemolytic streptococcus, which is very infectious, does not only infect the pharynx and does not only infect the tonsils, but at the same time in the pharynx and tonsils. It is common to be infected with group A beta hemolytic streptococcal pharyngitis and group A beta hemolytic streptococcal tonsillitis at the same time. • In other words, when group A beta hemolytic streptococcus is infected in the throat, that is, the pharyngeal mucosa, it cannot be infected only in the pharynx or only in the tonsils.
• So, it is common to simultaneously infect the pharynx and tonsils, causing infectious diseases to both sites at the same time, resulting in group A beta hemolytic streptococcal pharyngotonsillitis (Group A β hemolytic streptococcal pharyngotonsillitis). This is called viral pharyngotonsillitis.
• In addition, when an infectious disease occurs in the pharyngeal cavity due to a virus infection such as bacteria or adenovirus other than group A beta hemolytic streptococcus, the infectious disease does not occur separately only in the tonsils or the pharynx, and simultaneous infectious diseases occur in both the tonsils and the pharynx. is average.
• However, the name of group A beta hemolytic streptococcal tonsillitis caused by infection is called group A beta hemolytic streptococcal pharyngitis, group A beta hemolytic streptococcal pharyngitis, or group A beta hemolytic streptococcal tonsillitis.
• There are many cases where the doctors, patients, and parents are confused because they are often treated with different disease names. Here, these three disease names are actually almost the same medically.
Symptoms of group A beta hemolytic streptococcal pharyngeal tonsillitis
Photo 54. Group A beta hemolytic streptococcal pharyngitis and tonsillitis. Tonsils are swollen and red. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Photo 55. Group A beta hemolytic streptococcal pharyngitis and tonsillitis with swollen tonsils and red soft palate (pause of the mouth). Minor tonsillitis is not visible here. The white globules are stuck on the tongue. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Picture 56: Severe group A beta hemolytic streptococcal pharyngitis and tonsillitis. The tonsils were swollen and red and white. The uvula is red and swollen due to oophoritis. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Picture 57: Severe group A beta hemolytic streptococcal pharyngitis and tonsillitis. It was swollen and the red tonsils got stuck. Source-Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 58. Group A beta hemolytic streptococcal tonsillitis and pharyngitis With tonsillitis, both tonsils have become quite enlarged. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Photo 59. A group A beta hemolytic streptococcal tonsillitis and pharyngitis with slight swelling of both tonsils. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Picture 60. Group A beta hemolytic streptococcal infection can lead to tonsillitis and scarlet fever. As a symptom of scarlet fever, a white birch may form on the tongue, and then the tongue may temporarily change to a red tongue color similar to the color of a red strawberry. Source-Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 61: Group A beta hemolytic streptococcal infection in the tonsils and scarlet fever may also occur. At this time, as a symptom of scarlet fever, at first, a white birch may stick on the tongue, and then the tongue may change to a color similar to the color of a red strawberry. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Picture 62. Group A beta hemolytic streptococcal infection can occur in the tonsils and pharynx, and scarlet fever can also occur. The scarlet fever peeled off the stratum corneum of the skin of the palm. Source-Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Figure 63. Group A beta hemolytic streptococcal infection in the tonsils and scarlet fever can also occur. When you suffer from scarlet fever, you can get a rash on the skin similar to sandpaper.
The color of the skin rash is usually red. source; Used with permission from Health information service Merk Sharp & Dome, West Point, PA
Photo 64. Mucus is collected from the pharyngeal mucosa to test for group A beta hemolytic streptococcal bacterial culture or to test for emergency response to antibody antigens. Source-Copyright ⓒ 2012 John Sangwon Lee, MD. FAAP • Symptoms of group A beta hemolytic streptococcal pharyngeal tonsillitis differ depending on the age of the patient, the course of the disease, and the presence or absence of complications.
Typical symptom. signs of group A beta hemolytic streptococcal pharyngeal tonsillitis
• Tonsils become red, swollen, and enlarge with festering, and the throat hurts very much.
• mild to high fever,
• Symptoms such as headache, abdominal pain, and vomiting are present, and pain in the limbs and the whole body.
• It is common for the patient to be in a toxic state.
• If you look into the pharynx and tonsils with a light fixture, you can see that the tonsils, pharynx, and soft palate are red.
• Two to three days after the onset of this disease, it is easy to see white pus and mucus on the tonsils and large swollen tonsils.
• The lymph nodes in the neck just under the chin may swell, and touching them with your hands may hurt a little.
• This disease usually gets worse if not properly treated with appropriate antibiotics at the beginning.
• When it gets worse, the pharynx hurts more and more, and the sore throat is so severe that it is difficult to swallow saliva and food.
• Sometimes the child looks very sick, does not like to play, and tries to sleep only.
• It may be toxic.
• My appetite is low, so I don’t eat well, and I can’t sleep abnormally much or sleep well.
• Pharyngeal tonsillitis may occur as a result of an infection of group A beta hemolytic streptococcus, a fungus that produces flare-up toxins, and at the same time, scarlet fever.
www.drleepediatrics.com-Vol. 7 Pediatric and Adolescent Infectious Diseases-Refer to Scarlet Fever A group A beta hemolytic streptococcal pharyngeal tonsillitis is present, and a rash occurs on the skin, and white blotches on the tongue initially get stuck and then the tongue turns red, similar to the color of a red strawberry. In this case, acute pharyngeal tonsillitis is diagnosed with scarlet fever instead of a group A beta hemolytic streptococcal pharyngeal tonsillitis. Complications of group A beta hemolytic streptococcal infection Pharyngeal tonsillitis caused by group A beta hemolytic streptococcal infection can be life-threatening if not treated properly, and complications include: acute glomerulonephritis,• Rheumatic fever, www.drleepediatrics.com-Volume 11 Cardiovascular Disease in Children and Adolescents-Refer to Rheumatic Fever) • Rheumatic carditis,
• sepsis,
• otitis media,
• sinusitis,
• osteomyelitis,
• arthritis
• There are many other complications.
Diagnosis of group A beta hemolytic streptococcal pharyngeal tonsillitis
Figure 65. For bacterial culture of group A beta hemolytic streptococcus or group A beta hemolytic streptococcus antigen antibody aggregation, mucus is collected from the pharynx or the mucous membrane of the tonsils with a cotton swab. Source-Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Picture 66. After the mucus collected from the pharyngeal mucosa is buried in a blood-dried bacterium culture paper, the bacterial culture is placed in an incubator for culturing bacteria and cultured for 24 hours. These tests can also be easily done at a local hospital. The diagnostic accuracy is good, but the test costs are high. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Photo 67: Blood smeared slime culture paper (top) just before putting it into the bacteria culture incubator Bacterial culture paper grown with various bacteria other than group A beta hemolytic streptococcus (bottom left) Bacterial culture medium for blood grown by other types of research bacteria other than group A beta hemolytic streptococcus (how) A is taxo.
Taxo is an antibiotic disc used to culture and detect only group A among many types of streptococcus. Group A research bacteria cannot grow right around Taxo A, so it looks almost the same color as that of the original hemonucleus bacterium culture paper. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Picture 68: Group A beta hemolytic streptococcus did not grow in the blood in the bacterial culture incubator, but only various bacteria were grown (top). Only group A beta hemolytic streptococcus was grown in blood right aseptic cultures (bottom).
A is taxo. Taxo is an antibiotic disc used to culture and detect only group A among many types of streptococcus. Group A research bacteria cannot grow right around Taxo A, so it looks almost the same color as that of the original blood mucus bacterium culture paper. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Picture 70. Group A beta hemolytic streptococcus antigen antibody aggregation test was positive. When the antigen-antibody agglutination reaction test is performed with the new BioStar Strep A Ola Max rapid strep test, the test result is of 96% specificity diagnosis value. Therefore, it is not necessary to perform a group A beta hemolytic streptococcal culture test, and this test alone is said to be a sufficient condition to diagnose group A beta hemolytic streptococcal pharyngeal tonsillitis. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Picture 71. Group A beta hemolytic streptococcus culture in the hospital bacteriological laboratory. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
• If the disease is suspected by combining the medical history, symptoms, signs, and examination findings, mucus is collected from the pharyngeal mucosa or tonsil mucosa with a cotton swab, and a group A beta hemolytic streptococcus antigen antibody agglutination test is performed within 5-10 minutes. Can be diagnosed. (See photos 69 and 70.)
• Or, it can be confirmed within 24 hours by performing a group A beta hemolytic streptococcus bacterial culture test (Streptococcus culture test) with mucus on a cotton swab.
• If you have any of the symptoms and sore throats described above, you should look for viral pharyngeal tonsillitis or bacterial pharyngeal tonsillitis caused by group A beta hemolytic streptococci. When meningococcal bacteria are cultured in the pharyngeal mucosa swab collection specimen bacterial culture test
• When there is only pharyngitis, when mucus for a specimen is collected from the pharyngeal mucosa and a more detailed pharyngeal bacterial culture is performed in a hospital bacteriological laboratory, group A beta hemolytic streptococcus is also cultured and Neisseria meningitidis is also co-cultured.
• In this case, in general, meningococcal is treated as belonging to the group of normal organisms in the pharyngeal mucosa.
• Meningococcal pharyngitis is rarely caused by meningococcal pharyngitis. • Meningococcals grown in these bacterial culture tests are often considered clinically unreliable.
• Therefore, it is common to treat only pharyngitis caused by group A beta hemolytic streptococcus.
• In addition, when pharyngitis bacterial culture is tested at the local Pediatrics Department to determine if pharyngitis is caused by a group A beta hemolytic streptococcus infection, it is common to perform a bacterial culture test focusing only on group A beta hemolytic streptococcus in the pharyngeal bacterial culture test. It is (see photos 67 and 68).
Treatment of group A beta hemolytic streptococcal pharyngeal tonsillitis
• Group A beta hemolytic streptococcal pharyngeal tonsillitis is appropriately treated with one of penicillin, erythromycin, or cephalosporin antibiotics as prescribed by a doctor.
• Cephalosporins-based antibiotics include Cephalexin, Cephadroxil, Cefuroxime, Cefpodoxime, Cefprozil, Cefixime, Ceftibuten, and Cefdinir.
• It is said that treatment with one of them is more effective than treatment with penicillin ([Parents should also be anti-doctors-Encyclopedia of Pediatrics and Family Nursing)-Volume 7 Infectious Diseases for Children and Adolescents-see Table 1-10).
• Treatment of pharyngeal tonsillitis caused by viral infection with antibiotics does not have any therapeutic effect on the disease, and side effects may occur from such antibiotic treatment.
• For many other reasons, it should not be treated with antibiotics. • When treating pharyngeal tonsillitis caused by group A beta hemolytic streptococcal infection with antibiotics such as penicillin or erythromycin, the fever drops within 1 to 2 days after the start of treatment, and symptoms of sore throat and body pain almost disappear. is average.
• However, it must be taken during the recommended administration period of the prescribed antibiotics to eradicate group A beta hemolytic streptococcus to prevent recurrence of pharyngeal tonsillitis.
• The duration of treatment may differ depending on the type of antibiotic. • If you have a fever and your pharynx hurts, treat symptoms as needed with antipyretic analgesics such as Tylenol or Motrin/Ibuprofen.
• Physical rest should be taken until the fever has gone down and the pharynx no longer hurts.
• After 24 hours of starting treatment with appropriate antibiotics, symptoms generally improve and you may return to school as you gradually return to normal health.
• You don’t need to apply any medications to your pharynx, and you don’t necessarily have to get tonsillectomy surgery just because you have pharyngeal tonsillitis. See Tonsillectomy Surgery.
• Group A beta hemolytic streptococcus is highly infectious to others.
• Therefore, if someone in your household has a sore throat and fever, you should seek medical attention immediately.
• There is still no vaccine available to immunize against group A beta hemolytic streptococcal infection.
• Be sure to take all of the antibiotics for a certain period of time as prescribed by your doctor. Group A beta hemolytic streptococci that are resistant to antibacterial antibiotics (microrides)
• Group A beta hemolytic streptococci caused tonsillitis and pharyngitis have been well treated in the past with antibiotics such as penicillin or erythromycin, but nowadays group A beta hemolytic streptococcus has become resistant to microlide antibiotic treatment. Group A beta hemolytic streptococcal infections caused by tonsillitis and pharyngitis are not well treated with microlide antibiotics such as erythromycin, causing problems.
The American Infectious Disease Society’s Streptococcal Pharyngitis
Diagnosis and Treatment Guide Group A streptococcal (GAS) pharyngitis.Guidelines-Updated
• Diagnosed by rapid antigen-antibody aggregation test or by streptococcal bacterial culture test with pharyngeal mucus specimen
• If the result of the rapid antigen-antibody aggregation (reaction) test is negative in children and adolescents, confirm by conducting a streptococcal bacterial culture test with a pharyngeal mucus specimen.
• In adult patients, even if the result of the rapid antigen-antibody agglutination test is negative, it is not necessary to be confirmed by a streptococcal bacterial culture test with a pharyngeal mucus specimen.
• If you have signs of a viral infection, such as a cough, runny nose, or sores in your mouth, you may not need a streptococcal bacterial test.
• Infants and younger children under 3 years of age are not required to be tested for streptococcal bacteria unless their siblings have a streptococcal infection.
• If there is no allergen to penicillin, treat with Penicillin or Amoxicillin for 10 days.
• If you are allergic to penicillin, treat it with Cephalosporin, Clindamycin, Clarithromycin, or Azithromycin. Source: IDSA Infectious Diseases Society of America Issues Strep Guidelines September 2012
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd editio
- Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, harvey grant and robert murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
- The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
- Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
- Quick Reference To Pediatric Emergencies , Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Manual of Emergency Care
- 응급환자관리 정담미디어
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- Neonatal Resuscitation American heart Association
- Neonatology Jeffrey J.Pomerance, C. Joan Richardson
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
- Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
- Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- 소아과학 대한교과서
- 제1권 소아청소년 응급의료 참조문헌과 출처
- Other
Copyright ⓒ 2015 John Sangwon Lee, MD, FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”