호흡곤란, Breathing difficulty(Difficulty breathing)
호흡곤란의 개요
숨을 정상 이상으로 어렵게 쉬는 것을 호흡곤란이라 한다.
호흡곤란은 어떤 병의 증상 징후지 병명은 아니다.
호흡곤란의 정도에 따라 호흡곤란을
-
경도 호흡곤란,
-
중등도 호흡곤란,
-
중증도 호흡곤란으로 나눌 수 있다.
1. 경도 호흡곤란
-
숨 쉴 때 본인이 호흡곤란이 있는지도 모를 정도로 어렵게 숨을 쉬기도 하고,
-
숨쉬기 어렵다는 것을 본인이 느낄 수 있게 어렵게 숨을 쉴 때도 있다.
-
이때의 호흡곤란을 경도 호흡곤란이라고 한다.
2. 중등도 호흡곤란
-
경도 호흡곤란의 정도보다 더 심하고 중증도 호흡곤란의 정도보다 조금 덜 심한 호흡곤란을 중등도 호흡곤란이라고 한다.
-
중등도 호흡곤란 내지 중증도로 호흡곤란이 있으면 환아가 안절부절못하고 숨결이 빠르고, 숨을 깊게, 또는 얕게 쉬고, 상당히 힘들게 숨 쉬면서 괴로워 할 수 있다.
-
때로는 숨을 내쉴 때마다 가랑가랑 숨소리를 내거나 쌕쌕거리는 천명(Wheezing)을 낼 수 있고 숨을 들이 쉴 때 협착음(Stridor)을 낼 수 있다.
-
중증도 호흡곤란이 있을 때 적절한 치료를 즉시 해주지 않으면 생명이 위험할 수도 있다.
3. 중증도 호흡곤란
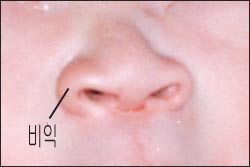
▴ 사진 1-210. 갓 태어난 신생아의 정상 코. 우 비익(콧방울),
폐렴이 있거나 호흡기에 이상이 있으면 호흡곤란이 생기고 숨 쉴 때마다 양쪽 콧방울이 벌렁벌렁 거릴 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
-
상당히 힘들고 어렵게 숨을 쉬면서 얼굴이 창백하고, 숨을 쉴 때마다 콧날개(콧방울/비익)가 벌렁벌렁 움직이고,
-
늑골 사이에 있는 늑골 근육이 흉강 속 쪽으로 딸려 들어갔다 바깥쪽으로 나왔다 하고
-
숨 쉴 때마다 두 어깨가 머리가 있는 위쪽으로 올라갔다 다리가 있는 아래쪽으로 내려갔다 할 수 있고,
-
숨이 금방 넘어갈 듯이 아주 어렵게 쉬어 옆에 있는 사람도 환아에게 호흡곤란이 있다는 것을 쉽게 알 수 있을 정도로 숨을 곤란하게 쉴 수 있다.
-
이 정도의 호흡곤란은 중증도 호흡곤란에 속한다.
호흡곤란의 원인
-
호흡곤란의 원인은 많다.
-
비강, 인두 강, 후두, 기관, 기관지 등 기도 속에 있는 이물이나, 폐, 심장, 횡격막, 또는, 신경, 근육 등에 생긴 어떤 병이나 어떤 이상으로 호흡곤란이 생길 수 있다.
-
다음 호흡곤란의 원인에 관해 더 구체적으로 설명한다.
-
입에 물고 놀던 장난감, 먹던 음식물, 또는 구토 물 등이 인두강, 후두, 기관, 또는 기관지 속으로 갑자기 들어가 이물로 인해 기도가 완전히 막힐 수도 있고, 부분적으로 막힐 수 있다. 이때 호흡곤란이 경도 내지 중등도 또 중증도로 심하게 생길 수도 있고 그 정도가 심하면 사망 할 수 있다.
-
갓 태어난 신생아의 비강의 후부(후비공)의 한쪽이나 양쪽이 선천적으로 완전히 막힐 수도 있고, 또는 일부가 후선천적으로 막힐 수 있다. 이런 선천성 후비공 폐쇄 기형을 선천성 후 비공 폐쇄증이라고 한다.
-
이런 선천성 후비공 기형을 갖고 태어난 신생아에게 호흡곤란이 심하게 생길 수 있다. 선천성 후 비공 폐쇄증이 비강의 후비공에 있을 때는 호흡곤란이 아주 심하게 생길 수 있고 중추성 청색증이 나타날 수 있다.
-
감기나 다른 종류의 상기도 감염병을 앓을 때 비강 속의 일부나 대부분이 완전히, 또는 일부가 일시적으로 막힐 때 호흡곤란이 생길 수 있다. 특히 신생아들이나 1~3개월 된 영아들이 감기에 걸리면 호흡곤란이 심하게 생길 수 있다([부모도 반의사가 되어야 한다–소아가정간호백과]-제6권 신생아 성장 발육 양호 질병–신생아 감기 참조).
-
후두 종양, 선천성 후두천명, 바이러스 후두염이나 크루프, 급성 박테리아 후두개염 등으로 하기도의 일부가 폐쇄될 때 호흡곤란이 생길 수 있다.
-
심장 비대나, 기관이나 기관지의 주위에 있는 장기나 종양 등으로 기관, 기관지, 또는 폐 등 호흡기가 압박될 때 호흡곤란이 생길 수 있다.
-
기관지 천식, 폐렴, 또는 세기관지염(모세기관지염) 등으로 호흡곤란이 생길 수 있다.
-
알레르기성 비염으로 비강 점막 층이 붓고 비강이 막힐 때 호흡곤란이 생길 수 있다.
-
폐기종, 긴장성 기흉 및 기흉, 무기폐, 심장병, 정신병 등으로 호흡곤란이 생길 수 있다.
-
그 외 다른 원인으로 호흡곤란이 생길 수 있다.
-
요약하면, 기도 내 이물, 급성 박테리아 후두개염, 급성 바이러스 후두염, 심한 기관지 천식, 급성 세기관지염, 급성 폐렴 등으로 소아청소년들에게 호흡곤란이 생길 수 있다.
호흡곤란의 응급치료
-
호흡곤란의 정도와 원인에 따라 응급치료를 한다.
-
숨이 많이 차고 아주 어렵게 숨을 쉬든지 거의 숨을 쉬지 못하면 사고 현장에서 응급처치를 바로 시작해야 한다.
-
필요에 따라 주위에 있는 사람들의 도움을 긴급히 청해서 서로 협력해 치료 한다.
-
그와 동시 의료구급대, 병원 응급실, 단골 소아청소년과 의사에게 긴급으로 전화해 그들의 지시에 따라 치료를 현장에서 시작한다.
-
호흡곤란이 상당히 심하고 의식이 있는 경우, 다른 사람의 도움을 받을 수 없으면 적절한 교통수단으로 병원 응급실로 급히 이송한다.
-
인두 속에 이물이 있다고 의심되고 의식이 있고 경미한 호흡곤란이 있을 때 의료구급대. 단골 소아청소년과 의사나 병원 응급실에 전화해 그들의 지시에 따라 현장에서 치료를 시작한다.
-
이물이 인두 속에 있고 이물을 쉽게 볼 수 있고 숨을 잘 쉴 수 있고 손가락 등으로 이물을 쉽게 꺼낼 수 있으면 손가락 등으로 이물을 꺼낼 수 있다.
-
인두 강 이물을 손가락으로 꺼낼 때 인두 강 속 이물이 후두 부분 기도 속 쪽으로 더 깊숙이 들어 갈 수 있고 또는 후두 부분 기도 속으로 더 깊이 들어갈 수 있고 그로 인해 후두 부분 기도 속이 완전히 막혀 질식할 수 있다.
-
이물이 인두 강 속에 깊숙이 있고, 숨쉬기가 곤란할 때 이물을 손가락으로 후벼서 꺼내기가 힘들 때도 많다.
-
환아를 안정시키면서 의료구급대이나, 단골 소아청소년과 의사나 병원 응급실에 긴급으로 전화해 그들의 지시에 따라 구급차나 다른 적절한 교통수단을 이용해 병원 응급실로 급히 이송해야 한다.
사진으로 보는 기도 내 이물 제거 응급 처치법

▴ 사진 1-211. 1.
이물이 인두강 속에 확실히 있거나, 있는지 몰라서 인두 강 속 이물이 있나 알아보기 위해 전등불을 비추면서 입안과 인두 강을 육안으로 들여다본다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

▴ 사진 1-212. 2.
입안이나 인두강 속에 있는 이물은 손가락으로 꺼낼 수 있으면 손가락으로 꺼낸다. 그러나 이물을 손가락으로 꺼내는 동안 잘못하면 인두 강 속 이물이 후두 부분 기도 속으로 더 깊숙이 들어가 기도가 완전히 막일 수도 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

▴ 사진 1-213. 3.
영유아의 기도가 이물로 막혀 숨을 쉬지 못하는 순간이나 숨을 더 이상 쉬지 못하는 순간에는 양쪽의 견갑골 사이 등 부분을 손바닥으로 5번 정도 연달아 처 기도 내 이물 제거 등치기 처치를 한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

▴ 사진 1-214. 4.
그래도 영유아의 기도 속 이물이 기도 속에서 나오지 않으면 위 사진과 같이 두 손가락으로 앞가슴을 미는 기도 내 이물 제거 처치를 한다. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
▴ 사진 1-215. 6.
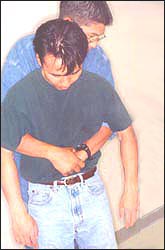
기도 속 이물로 숨이 막혀 숨을 전혀 쉴 수 없는 순간에는 하임리크 처치법으로 기도 속 이물제거 응급처치를 할 수 있다. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

▴ 사진 1-216. 5.
기도 속 이물로 숨이 막혀 숨이 막 넘어가려고 할 때나 금방 숨이 넘어갔을 때는 편평한 바닥에 눕히고 손바닥으로 오목가슴을 흉강 속 쪽을 향해 민다.Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
인두 강 속 이물로 금방 질식되어 곧 사망할 것 같고 호흡곤란이 극히 심하고 다른 사람의 도움을 구할 수 없는 상황에 처해 있을 때의 기도 내 이물제거 응급처치
-
안전한 장소에 영아를 옮긴다.
-
상체를 하체보다 15∼30°낮게 눕히든지
-
영아의 얼굴이 바닥을 향해 엎드린 자세로 처치자의 무릎 위에 눕히든지 앉힌 다음
-
영아의 양쪽 견갑골의 사이 부분을 손바닥으로 5번 연달아 세게 치는 기도 속 이물 제거 처치를 한다.
-
영아기 이후 유아들이나 학령기 아이들의 기도 내 이물이 있을 경우는, 아이가 서 있는 자세에서 오목 가슴을 미는 기도 내 이물 제거 오목 가슴 밀기 하임리크 처치법으로 기도 속 이물제거 응급처치를 한다.
-
또는 바닥에 등을 대고 눕힌 후 사진 286에서 보는 것같이 기도 내 이물 제거 앞가슴 밀기 처치를 하든지 기도 내 이물 제거 오목가슴 밀기 처치법을 할 수 있다.
-
더 자세한 기도 내 이물 제거 처치법은 ‘기도 속에 이물이 들어갔을 때‘를 참조한다.
-
이런 처치를 하는 중 인두 강 내 이물이 입 밖으로나 입안으로 기도 속에서 나올 수 있고 후두 부분 기도 속으로 더 들어가 기도가 더 막혀 생명이 더 위험할 수 있다(p.00 기도 속에 이물이 들어갔을 때 참조).
-
급성 박테리아 후두개염으로 호흡곤란이 심하고 목이 쉬고 고열이 나며 인두 통 등의 증상 징후가 있을 수 있다.
-
급성 박테리아 후두개염이 있다고 의심되면 의료구급대, 단골 소아청소년과 의사, 또는 병원 응급실에 응급으로 전화해 그들의 지시에 따라 치료한다.
-
가능하면 소아청소년과 전문의, 이비인후과 전문의, 외과 전문의, 마취과 전문의의 도움을 즉시 받을 수 있는 최 인근 종합 병원 응급실로 구급차나 다른 적절한 방법으로 급히 데리고 가야한다([부모도 반의사가 되어야 한다–소아가정간호백과]-제8권 소아청소년 호흡기 질환–급성 후두개염에 의한 크루프 참조).
-
심한 기관지 천식, 급성 세기관지염, 또는 폐렴 등으로 숨이 차고, 호흡이 곤란할 때 의료구급대, 병원 응급실, 단골 소아청소년 의사의 지시에 따라 치료한다.
-
가능하면 어떤 원인으로 인해 호흡곤란이 생겼나 알아 그 원인에 따라 현장에서 호흡곤란의 정도와 원인에 따라 적절히 치료한다.
-
호흡곤란이 아주 심하거나, 숨을 거의 쉬지 못하거나, 무호흡 상태의 증상 징후가 있을 때나 맥박이 뛰지 않을 때는 처치자의 입을 환아의 입에다, 또는 입과 콧구멍 두 부분에 대고 인공호흡을 하고 심장마사지를 하는 심폐 소생술을 한다.
Breathing difficulty(Difficulty breathing) 호흡곤란
Overview of Difficulty Breathing
- Breathing more difficult than normal is called dyspnea.
- Difficulty breathing is a symptom of a disease, not a disease name.
Depending on the degree of dyspnea
- Mild dyspnea,
- Moderate difficulty breathing,
- Severe can be divided into shortness of breath.
1. Mild breathing difficulties
- When your child breathes, your child breathes so hard that you don’t even know if your child has had difficulty breathing, Sometimes breathing is difficult so your child can feel that it is difficult to breathe.
- Difficulty breathing at this time is called mild dyspnea.
2. Moderate breathing difficulties
- Difficulty breathing is more severe than the degree of mild dyspnea and a little less than the degree of severe dyspnea is called moderate dyspnea.
- If the child has moderate to severe shortness of breath, the child may feel restless, breathe quickly, breathe deeply, or shallowly, and may suffer from breathing very hard.
- Sometimes, each time you exhale, you can make stridor or wheeze, and you can make stridor when you inhale. Severe breathing difficulties can be life-threatening if appropriate treatment is not given immediately.
3. Severe difficulty breathing
▴ Photo 1-210. The normal nose of a newborn baby. Right-wing (alar nose).
If your child has pneumonia or has respiratory problems, your child may have difficulty breathing and your child’s noses may flutter each time you breathe. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- The face is pale while breathing quite hard and difficult, and the nose wings (alar nose) move around each time you breathe,
- It is said that the rib muscle between the ribs rolls into the chest cavity and comes out. With each breath, both shoulders rise above, the head up-down.
- It is very difficult to breathe quickly, so even the person next to you can have difficulty breathing so that it is easy to know that the patient has difficulty breathing.
- This degree of dyspnea belongs to severe dyspnea.
Causes of dyspnea
- There are many causes of dyspnea.
- A foreign body in the airways such as the nasal cavity, pharyngeal cavity, larynx, trachea, bronchi, etc., lungs, heart, diaphragm, or nerves, muscles, etc., may cause breathing difficulties.
- Next, explain the cause of dyspnea in more detail. Toys, food, or vomiting water that was used to play with the mouth may suddenly enter the pharyngeal cavity, larynx, trachea, or trachea, and the airway may be completely blocked or partially blocked by a foreign body.
- At this time, shortness of breath may occur with mild to moderate or severe severity, and if the degree is severe, death may occur.
- One or both of the posterior parts of the nasal cavity of a newborn baby (posterior nostril) may be congenital and completely blocked, or some may be a congenital blockage.
- This congenital posterior nostril obstruction is called post congenital nostril atresia(Choanal atresia). Newborns born with these congenital posterior nostril malformations can have severe breathing difficulties. When congenital nostril obstruction is present in the posterior nostril of the nasal cavity, dyspnea can develop very severely and central cyanosis can occur.
- When suffering from cold or other types of upper respiratory infections, breathing difficulties may occur when part or most of the nasal cavity is completely or partially blocked. In particular, if newborns or infants aged 1 to 3 months have a cold, breathing difficulties can occur severely ([Parents should also be at least the half-doctors-Encyclopedia of Pediatrics and Family Nursing)-Volume 6, Newborn’s Growth and Developmental Diseases-Newborn Colds).
- Difficulty breathing may occur when part of the lower respiratory tract is obstructed due to a laryngeal tumor, congenital laryngeal wheezing, viral laryngitis or croup, or acute bacterial epiglottis.
- Difficulty breathing may occur when the respiratory tract, such as the trachea, bronchi, or lung, is compressed due to an enlarged heart or organs or tumors around the trachea or bronchi. Difficulty breathing may occur due to bronchial asthma, pneumonia, or bronchiolitis (capillary bronchitis).
- With allergic rhinitis, swelling of the nasal mucosa and clogging of the nasal cavity can cause dyspnea.
- Difficulty breathing may occur due to emphysema, tense pneumothorax and heart disease, and mental illness.
- Difficulty breathing can be caused by other causes. In summary, breathing difficulties can occur in children and adolescents due to foreign bodies in the airways, acute bacterial epiglottis, acute viral laryngitis, severe bronchial asthma, acute bronchiolitis, and acute pneumonia.
Emergency treatment for dyspnea
- Emergency treatment is given depending on the degree and cause of dyspnea.
- If your child has a lot of breath and breathes very hard or hardly breathes, first aid should be started immediately at the scene of the accident.
- If necessary, urgently seek help from people around them, and cooperate with each other to treat them.
- At the same time, urgently call medical paramedics, hospital emergency rooms, and regular pediatricians, and follow their instructions to begin treatment on the spot.
- If breathing difficulties are quite severe and your child is conscious,
- if you cannot get help from other people, you must promptly transfer them to the hospital emergency room by means of appropriate transportation.
- Medical paramedics when suspected of having a foreign body in the pharynx, conscious and mild breathing difficulties.
- Call your regular pediatrician or hospital emergency room and follow their instructions to begin treatment on the spot.
- If the foreign body is in the pharynx, you can easily see the foreign body, breath well, and you can easily remove the foreign body with your finger, you can remove the foreign body with your finger or the like.
- When the pharyngeal foreign body is pulled out with a finger, the foreign body in the pharyngeal cavity can go deeper into the laryngeal airway or deeper into the laryngeal airway, which can completely block the occipital airway and cause suffocation.
- When the foreign body is deep in the pharyngeal river and is difficult to breathe, it is often difficult to pull it out with a finger. While stabilizing the child, you must call a medical paramedic, a regular pediatrician, or hospital emergency room in an emergency and follow their instructions to urgently transfer them to the hospital emergency room using an ambulance or other appropriate means of transportation.
First aid method to remove foreign objects in the airways shown in the picture
▴ Photo 1-211. 1. If you don’t know if the foreign body is in the pharyngeal cavity, so you may look into my mouth and pharyngeal cavity, with the naked eye while lighting light to see if there is any foreign material in the pharyngeal cavity, Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
▴Photo 1-212. 2. Foreign objects in the mouth or pharyngeal cavity can be pulled out with a finger if it can be pulled out with a finger. However, if you make a mistake while pulling the foreign body out with your finger, the foreign body in the pharyngeal cavity may go deeper into the laryngeal airway and completely block the airway. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
▴ Photo 1-213. 3. At the moment when the infant’s airway is blocked with a foreign object and cannot breathe or can no longer breathe, the back slaps between the shoulder blades on both sides is successively carried out with the palm of the hand 5 times to remove the foreign body in the airway. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
▴ Photo 1-214. 4. Still, if the foreign body in the airway of the infant does not come out of the airway, remove the foreign body in the airway by pushing the chest with two fingers as shown in the picture above. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
▴ Photo 1-215. 6. At the moment when you can’t breathe at all because your child are choked by a foreign body in the airway, you can take first aid to remove the foreign body in the airway with the Heimlique treatment method. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
▴ Photo 1-216. 5. When your child is choking with a foreign body in your airways, or when he is about to suffocate, or when he has just passed out of breath, lie on a flat surface and push your concave chest toward the chest cavity with your palms. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
First aid to remove foreign bodies in the airways when you are in a situation where your child is suffocated by a foreign body in the pharynx and he is likely to die soon, and he has very severe breathing difficulties and you cannot seek help from other people.
- Move the infant to a safe place.
- Either lay the upper body 15-30° lower than the lower body
- Put the infant’s face down on the person’s lap with the face facing the floor or sit down
- Perform a treatment to remove foreign bodies in the airways by slapping the infant’s shoulder blades between the two shoulder blades 5 times in a row with the palm of the hand.
- If there is a foreign body in the airways of infants or school-age children after infancy, the child is in a standing position, pushing the epigastrium,
- removing the foreign material in the airway, pushing the concave chest. Alternatively, as shown in Picture 286,
- after lying on the floor with your back,
- you can either remove the foreign body in the airway, or do they push on the front chest or remove the foreign body inside the airway, and use the concave breast push treatment method.
- For more details on how to remove foreign objects in the airways, refer to when a foreign body enters the airways’. During these treatments, foreign objects in the pharyngeal cavity may come out of the mouth or into the airways,
- and further into the laryngeal part of the airways, the airways may become more blocked and life may be more dangerous (p. Reference).
- Acute bacterial epiglottis infection may have symptoms such as severe breathing difficulties, a sore throat, high fever, and a sore throat.
- If you suspect that you have acute bacterial epiglottis, call a medical paramedic, a regular pediatrician, or hospital emergency room as an emergency, and treat them according to their instructions.
- If possible, you should take an ambulance or other appropriate method to the emergency room of the nearest general hospital where you can immediately get help from a pediatrician, otolaryngologist, surgeon, and anesthesiologist
- (Parents should also be at least the half -doctors- Pediatric and Family Nursing Encyclopedia]-Volume 8 Child and Adolescent Respiratory Disease-See Croup due to Acute Epiglottitis).
- If your child is short of breath due to severe bronchial asthma, acute bronchiolitis, or pneumonia, or has difficulty breathing, treat according to the instructions of a medical paramedic, hospital emergency room, or a regular pediatrician.
- If possible, find out which cause caused dyspnea.
- Depending on the cause, treat it appropriately according to the degree and cause of dyspnea at the site.
- When breathing difficulties are very severe, when there is almost no breathing, or when there are symptoms of apnea, or when the pulse is not beating, place the patient’s mouth in the patient’s mouth, or in both the mouth and nostrils, perform artificial respiration, and perform heart massage. Do cardiopulmonary resuscitation
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
-
심폐 소생술(CPR)
-
신생아 심폐 소생술
-
콧구멍 속 이물,(비강 속 이물), 외비공의 이물
-
기도 속에 이물이 들어갔을 때와 질식
-
기도 내 이물 제거 하임리크 처치법
-
생선가시가 목구멍 속에 걸렸을 때
-
소화기 속 이물, 소화관 내 이물, 위장관 내 이물
-
질식
-
Manual of emergency pediatrics 5th edition, Robert M. Reece, M.D., p.20
-
Manual of emergency pediatrics 4th edition, Robert M. Reece, M.D., p.8
-
Quick Reference to Pediatric Emergencies, Delmer J. Pascoe, M.D., p.39
-
Emergency care and transportation of the sick and injured, 3rd edition, American Academy of orthopedic surgeons. p.77
-
Nelson textbook, 14 edition p.265-226
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과-부모도 반의사가 되어야 한다, 이상원 저
-
The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
-
Preparation for Birth. Berverly Savage and Dianna Smith
-
임신에서 신생아 돌보기까지. 이상원
-
Breastfeeding. by Ruth Lawrence and Robert Lawrence
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th-31st Ed 2021
-
Nelson Text Book of Pediatrics 19th-21st Edition
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
Growth and Development of Children, George H. Lowrey 8th edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
others
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”