코피가 날 때(비출혈), Nose bleeding(Epistaxis)
비출혈의 개요
- 누구도 일생동안 적어도 한두 번 정도 코피를 흘렸던 경험이 있다.
- 코를 풀 때 휴지에 조금 묻을 정도로 코피가 조금 날 수도 있고 코피가 줄줄 흘러나올 정도로 많이 날 때도 있다.
- 코피가 생명을 위험할 정도로 많이 나는 경우는 아주 드물다.
- 코피는 어떤 병의 증상 징후이지 병명은 아니다.
- 코피가 나면 코피를 나게 하는 원래 병을 찾아 그 병에 따라 코피를 치료해야 한다.
비출혈의 원인
- 비강을 좌우 양쪽 비강으로 나누는 격막이 있다. 이 격막을 비중격이라고 한다.
- 비중격의 표면을 덮고 있는 양쪽 비중격 점막층은 비강의 다른 부분을 덮고 있는 점막층과 같은 종류이다.
- 비강의 비중격을 덮은 점막층 하 조직에는 정상적으로 모세혈관들이 많이 분포되어 있다.
- 비중격의 앞 부위의 점막층에는 비강 다른 부위의 점막층 보다 특별히 더 많은 모세혈관이 정상적으로 모여있다.
- 모세혈관들이 특별히 더 많이 모여있는 비강 점막 층의 아래 조직 비강 부위를 “키셀바흐 삼각 부위”라 한다(그림 211 참조).
- 키셀바흐 삼각 부위 얼기(Kiesselbach’s trigone plexus)에 있는 점막층 모세혈관들은 콧구멍 속을 손가락 끝으로 후빌 때나 재채기할 때, 또는 코를 살짝 비빌 때도 쉽게 터질 수 있다.
- 특히, 손가락 끝으로 콧구멍을 후빌 때는 비강 점막층과 그 아래 점막층 조직에 쉽게 상처를 입을 수 있고 그 부위에 있는 모세혈관이 터져 비출혈이 더 쉽게 나 코피가 나는 때가 많다.
- 알레르기성 비염이 있을 때 그로 인해 비강 점막층에 비염이 생길 수 있고, 또 비강 점막층에 있는 모세혈관과 점막층 아래에 있는 조직 모세혈관들이 급성으로 충혈되거나 또는 만성으로 충혈되어 있는 것이 보통이다.
- 알레르기성 비염으로 코가 가려울 때 환아가 무의식적으로 콧구멍 속을 자주 후비거나, 코를 자주 문지르거나, 재채기를 할 수 있다. 이때 비강 점막층에 있는 충혈된 모세혈관과 점막층 조직에 있는 모세혈관이 쉽게 터지고 거기서 코피가 쉽게 자주 날 수 있다.
- 어떤 때는 콧구멍 속을 후비지도 않고 뚜렷한 코피가 날 이유를 확실히 찾을 수 없는데도 코피를 자주 흘린다.
- 감기나 그외 다른 종류의 바이러스 상기도염이나 알레르기성 비염 등을 앓을 때 비강 점막층에 염증이 생기고 비강 점막층의 모세혈관이 충혈되고 터지면 코피가 쉽게 날 수 있다.
- 특히 감기나 감기 이외 상기도 바이러스 감염이 있을 때나 알레르기성 비염이 있을 때 비강 점막층에 염증이 생기고 비강 점막층 하 조직에 있는 모세혈관이 잘 터져서 코피가 날 수 있다.
- 알레르기성 비염 등으로 생긴 코딱지가 비강 점막층을 오랫동안 자극 할 때,
- 실내 온도가 높고 건조할 때,
- 비강 점막층이 마르고 점막층 하 조직 모세혈관이 비정상적으로 확장될 때
- 비강 점막층이 마르고 점막층 하 조직 모세혈관이 더 잘 터질 수 있다.
- 이럴 때 재채기나 기침을 조금만 해도, 코를 무의식적으로 살짝 문지르거나 콧구멍 속을 후빌 때도 비강 점막층에 있던 모세혈관이 터져서 코피가 날 수 있다.
- 잘못해서 코 타박상을 입으면 비강 점막층의 모세혈관이 터져 코피가 날 수 있다.
- 그 외 다른 여러 가지 원인에 의해 코피가 날 수 있다.
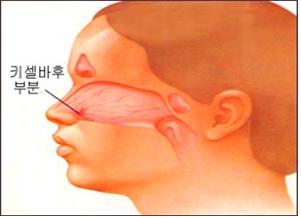
▴ 그림 1-23. 비강 점막층과 점막층 하 조직에 있는 모세혈관.
a-비강 점막층과 그 아래에 있는 키셀바흐 삼각 부위.
비강 점막층의 모세혈관이나 점막층 아래 조직층에 있는 모세혈관이 터지면 코피가 날 수 있다. Shearing corporation, Kenilworth, N.J. USA 과 소아가정간호백과
비출혈의 진단
- 코피가 나는 사실을 목격하고 쉽게 진단할 수 있다.
- 때로는 밤에 자다가 코피가 나서 비강 맨 뒤쪽 부위(후비강 부위와 비인두 부위)쪽으로 흘러 목구멍 속으로 들어간 코피를 삼킬 수 있다. 이렇게 무의식적으로 삼킨 피를 갑자기 뱉거나 토할 때도 있다. 뒤 늦게 밤중에 코피를 흘렸다는 사실을 아침에 알고 간밤에 코피가 났었다고 진단할 수 있다.
- 콧구멍과 비강 속을 비경이나 비 내시경으로 들여다보고 코피가 나는 점막층의 부분을 쉽게 찾아서 비출혈을 진단할 수 있다.
- 전신 출혈성 질환으로 코피가 나면 CBC 혈액 검사와 출혈의 원인을 알아보기 위해 하는 출혈 스크린 검사 등을 해서 코피가 나는 원인을 찾아 진단해야 할 때도 있다(표23 참조).
비출혈의 치료
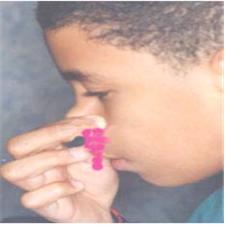
▴ 사진 1-169. 코피가 날 때 머리를 뒤로 젖히지 말고 앞으로 조금 살짝 숙이고 두 손가락 끝으로 코앞부위(비익)를 사진에서 보는바와 같이 잠시 동안 꼭 잡으면 코피가 멎는 것이 보통이다. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- 코피를 나게 한 원인과 정도 등에 따라 치료한다.
- 코를 풀 때마다 코피가 가끔 조금 나면 코를 세게 풀지 않도록 한다.
- 알레르기성 비염, 또는 감기나 다른 종류의 바이러스 호흡기 감염으로 코피가 조금 날 수 있다. 이때는 그 병이 다 나으면 코피가 더 이상 나지 않든지, 그 후 가끔 조금씩 나다가 자연히 그치는 것이 보통이다.
- 코피가 날 때는 코피가 비강 맨 뒤 후부(후비공)를 통해 인두 강 쪽으로 흘러 들어가지 않도록 머리를 앞으로 조금 숙여야 한다. 그와 동시에 엄지와 집게손가락 끝으로 코의 말랑말랑한 앞부분(비익)을 약 5~10분간 꼭 잡으면 대부분의 코피는 자연히 멈춘다.
- 코피가 비강 맨 뒤 부위로 흘러서 인두 강 쪽으로 흘러온 코피를 삼키지 말고 뱉어야 한다.
- 찬 물수건이나 얼음물 주머니를 콧등 위에 2~3분간 올려놓으면 비강 점막 층 모세혈관이 수축되어 코피가 더 빨리 멈출 수 있다.
- 이런 식으로 코피를 1차 응급처치해도 코피가 멎지 않고 계속 많이 나거나 자주 나면 단골 소아청소년과나 병원 응급실에 전화해서 그들의 지시에 따라 치료한다.
- 과거에 코피를 한 번이라도 많이 흘린 적이 있거나 코피가 그치지 않고 계속 났던 경험이 있는 환아가 코에 외상을 입은 후 코피가 계속 날 때는 의료구급대, 병원 응급 의료실, 또는 단골 소아청소년과에 응급으로 전화해 그들의 지시에 따라 치료한다.
- 알레르기성 비염을 앓는 환아들의 대부분은 코피를 더 자주 흘릴 수 있다. 알레르기성 비염을 적절히 치료해 주면 코피가 덜 나는 것이 보통이다.
- 알레르기성 비염이나 다른 종류의 비염 등이 있을 때 코딱지가 비강 점막에 더 자주 생길 수 있고 코딱지가 비강 점막 층에 오랫동안 붙어 있을 수 있다. 코딱지로 비강 점막 층 모세혈관이 자극되어 모세혈관이 터져 코피가 자주 날 수 있다. 이때 의사의 처방에 따라 비강 점막층에 박트로반(Bactroban ointment/mupirocin ointment) 항생제 연고나 배시트라신 항생제 연고나 크림을 1일 3회, 10일간 발라주면 비출혈이 더 이상 나지 않을 수 있다.
- 실내온도가 보통 이상으로 높든지 습도가 아주 낮고 비강 점막 층이 건조하면 코피가 더 자주 날 수 있다. 이때는 실내온도와 습도를 알맞게 적절히 조절해야 한다.
- 코피가 자주 나거나 계속 날 때는 집에서 부모가 일차 응급치료를 한 다음 의사의 추적 진단 치료를 받아야 한다. 어떤 때는 비강 점막 층의 모세혈관의 일부를 질산은봉으로 지져 치료한다.
- 아드레날린 몇 방울을 면구에 묻혀 비강 속에 잠시 동안 넣었다가 제거 하면 코피가 멈출 수 있다(아드레날린은 혈관수축 작용이 있는 약이다).
- 혈소판 감소증, 백혈병, 또는 다른 여러 가지 원인으로 나는 코피는 그 원인에 따라 치료한다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제18권 소아청소년 이비인후 질환-비출혈 참조
|
다음은 “코피가 자주 나요...”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 코피가 자주 나요...
Q.
7살 된 남자아이 입니다. 어릴 때부터 감기로 병원을 자기 집 들르다시피 했어요. 5살부터는 소아청소년과에서 이비인후과로 옮겨 다니고 있습니다. 비염이 있어 코가 약해 코피가 날수 있다는 건 알고 있어요. 하지만 너무 자주(한 달에 한 번꼴) 흘려요. 다른 아이들에 비해. (저는 태어나서 한 번도 코피를 흘린 적이 없는데…) 조금 나다 말면 별 걱정이 없을 텐데. 이건 정말 코피인지 알 수 없을 정도로 줄줄 흘러, 보는 사람이 질겁할 정도예요. 병원에서는 별것 아니라고 하지만 제가 보기에는 곁으로 코에 이상이 있을 때 ‘감기가 걸렸다든지‘ 할 경우에는 코피를 안 흘려요. 어린이 집에서는 조금씩 정도밖에는 안 흘린데요. 근데 이상하게도 잠자다 ‘엄마 나 코피나‘할 때 보면 엄청 많이 흘려요. 정말 비염 때문에 다른 아이들보다 자주 코피를 흘리는 걸까요???
A.
승원님께
안녕하십니까. 질문해 주셔서 감사합니다.
자녀의 나이와 성별, 과거 현재 가족의 병력, 증상 징후와 진찰소견, 적절한 임상검사 등의 결과를 종합해서 진단 치료하는 것이 이상적이지만 주신 정보를 참작해서 답변을 드립니다.
만일 아드님을 제 소아청소년과로 데리고 오신다면 과거 가족 병력을 들어 보고 알레르기 병력, 성장 발육 과정, 임신 출생 병력, 습관, 그외 더 자세한 병력을 들어보고 머리끝부터 발끝까지 신체검사를 하겠습니다.
특히 비경이나 비 내시경으로 비강을 들여다보겠습니다.
신체검사에서 피부에 출혈 반점이 없고 비강 속에 별 이상이 없거나 비강 점막 층이 창백해 보이고 눈 밑에 알레르기 샤이너가 있고 과거에 천식이나 알레르기성 비염을 앓았던 병력이 있고 친 부모 형제 재매들에게도 알레르기성 질환이 있는 가족 병력이 있으면 아드님에게 자주 나는 코피는 알레르기성 비염으로 생길 가능성이 가장 많다고 진단하겠습니다.
때로는 알레르기성 비염과 축농증이 같이 있는 경우도 많습니다.
신체검사의 결과가 정상이고 부모가 아드님의 코피 때문에 걱정을 많이 하시고 세 번 이상 저의 소아청소년과에 상담하러 오시면 CBC 혈액 검사, 출혈의 원인을 알아보기 위해 하는 출혈 스크린 검사(Bleeding screening test)(표23 참조)를 해서 전신 출혈성 질환이 있나 알아보겠습니다.
이런 검사는 비교적 간단한 피검사이고 피의 응고가 잘 되는지 알아보는 검사입니다.
검사의 결과가 정상이면 이비인후과에 보내서 이비인후과 전문의 의견도 들어보겠습니다.
이비인후과 전문의에게 의뢰하겠습니다.
의뢰 받은 이비인후과 전문의가 자녀의 코피는 알레르기성 비염으로 난다고 진단을 하고 저에게 아드님을 다시 보내면서 저보고 계속 알레르기성 비염을 치료하라고 하시면 자녀의 알레르기성 비염을 알레르기성 비염을 유발시킬 수 있는 항원 제거나 항원 피함 등 환경 정리 치료방법으로 치료하고 비강 분무용 스테로이드제, 제 2세대 항히스타민제 등으로 치료하라고 저에게 제시하면 저도 이비인후과 전문의 치료방법에 따르겠습니다.
자녀의 코피를 치료할 때는 자녀와 부모와 함께 상담해서 그 자녀의 병에 가장 좋은 치료 방법을 물론 선택해서 치료하겠습니다.
이상 말씀드린 것을 참고로 해서 치료를 해 보십시오.
[부모도 반의사가 되어야 한다–소아가정간호백과]-제15권 소아청소년 알레르기 및 자가 면역질환–알레르기성 비염, 제18권 소아청소년 이비인후 질환–코피(비출혈) 등을 참조하시기 바랍니다. 그리고 질문이 더 있으시면 다시 연락해 주시기 바랍니다. 감사합니다.이상원 드림
Nose bleeding (Epistaxis) 코피가 날 때(비출혈)
Overview of nose-bleeding
- Everybody has ever had nosebleeds at least once or twice in their lifetime.
- When you blow your nose, you may bleed a little so that you put a little bit of tissue on it, or there are times when there are so many times that your nose bleeds out in a row.
- It is very rare that a nosebleed is life-threatening.
- A nosebleed is a symptom of a disease, not a disease name.
- If you have a nosebleed, you need to find the original disease that caused the nosebleed and treat the nosebleed according to the disease.
Causes of nasal bleeding
- There is a septum that divides the nasal cavity into left and right nasal passages.
- This septum is called the nasal septum.
- Both sides of nasal septum mucosa covering the surface of the nasal septum are of the same type as the mucous membrane covering other parts of the nasal cavity.
- Capillaries are normally distributed in the tissue under the mucous layer covering the nasal septum. In the mucous layer in front of the nasal septum, more capillaries are normally collected than in the other areas of the nasal cavity.
- The tissue nasal region below the nasal mucosa layer, where capillaries are particularly concentrated, is called the “Kiselbach triangular region” (see Figure 211).
- The capillaries in the mucosa in the Kisselbach’s trigone plexus can easily explode when swiping through the nostrils with a fingertip, sneezing, or gently rubbing the nose. In particular, when opening the nostrils with the tip of a finger, the nasal mucosa layer and the tissue underneath the nasal mucosa can be easily injured, and the capillaries in the area rupture, causing nasal bleeding more easily or nosebleeding.
- When allergic rhinitis is present, it may cause rhinitis in the nasal mucosa, and capillaries in the nasal mucosa layer and tissue capillaries under the mucous layer are usually congested acutely or chronically. When the nose is itchy due to allergic rhinitis, the child may unconsciously rub the inside of the nostrils frequently, rub the nose frequently, or sneeze.
- At this time, the congested capillaries in the nasal mucosa layer and the capillaries in the mucous layer tissue easily burst, and there may be frequent nosebleeds.
- Sometimes, your child can bleed frequently, even though your child doesn’t even go through your child’s nostrils and your child can’t find out for sure why he has a distinct nosebleed.
- When suffering from cold or other types of viruses such as upper respiratory tract infection or allergic rhinitis, the nasal mucosa becomes inflamed and the capillaries in the nasal mucosa become congested and burst, which can lead to nosebleeding easily.
- In particular, when there is an upper respiratory viral infection or allergic rhinitis other than a cold, the nasal mucosa is inflamed, and capillaries in the tissues under the nasal mucosa are easily ruptured, resulting in nosebleeding.
- When snot caused by allergic rhinitis etc. irritates the nasal mucosa for a long time,
- When the room temperature is high and dry,
- When the nasal mucosa is dry and the submucosal tissue capillaries are abnormally expanded, the nasal mucosa may dry out and the tissue capillaries under the mucous layer may rupture better.
- In this case, even a little sneezing or coughing, involuntarily rubbing your nose or blowing in your nostrils can cause the capillaries in the nasal mucosa to burst and cause nosebleeds.
- Accidental nasal bruises can cause capillaries in the nasal mucosa to burst and cause nosebleeds.
- There are many other causes that can cause nosebleeds.
▴ Figure 1-23. Capillaries in the nasal mucosa and submucosa. a-the layer of the nasal mucosa and the area of the Kisselbach triangle below it. If the capillaries in the nasal mucosa or the capillaries in the tissue layer below the mucous membrane burst, nosebleeds may occur.
Shearing corporation, Kenilworth, N.J. Department of USA Department of Child and Family Nursing Encyclopedia Diagnosis of non-bleeding
- It’s easy to see and diagnose nosebleeds.
- Sometimes, while sleeping at night, the nose bleeds and flows to the back of the nasal cavity (the posterior nasal cavity and the nasopharynx) and swallows the nosebleed into the throat.
- There are also times when you suddenly spit or vomit blood that you swallowed unconsciously.
- You can diagnose that your child had a nosebleed late at night after knowing in the morning that you had a nosebleed late at night.
- Nasal bleeding can be diagnosed by looking into the nostrils and nasal cavity with a parenteral or nasal endoscope, and easily finding the part of the mucous layer where the nose is bleeding.
- When a nosebleed occurs due to a systemic bleeding disease, it is sometimes necessary to diagnose the cause of the nosebleed by performing a CBC blood test and a bleeding screen test to determine the cause of the bleeding (see Table 23).
Treatment of nose-bleeding
▴Photo 1-169. When you have a nosebleed, do not tilt your head backward, bend it slightly forward, and hold the front part of the nose (alar nose) with two fingertips for a while, as shown in the picture, to stop the nosebleed. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- Whenever you blow your nose, try not to blow your nose hard if you occasionally bleed a little.
- Allergic rhinitis or a cold or another type of viral respiratory infection can cause minor nosebleeds.
- At this time, it is common for the nose to bleed to stop when the disease is healed, or occasionally come out little by little after that, and then stop spontaneously.
- When you have a nosebleed, you need to bend your head slightly forward so that the nosebleed does not flow into the pharyngeal cavity through the posterior part of the nasal cavity (posterior nostril).
- At the same time, most of the nosebleeds will stop naturally if you hold the soft front part (alar nose) of the nose with the tip of your thumb and forefinger for about 5 to 10 minutes.
- Nose bleeding flows to the back of the nasal cavity and should be spitting out rather than swallowing.
- Putting a cold wet wipe or a bag of ice water on your nose for 2-3 minutes can constrict the capillaries in the nasal mucosa and stop bleeding more quickly.
- In this way, even if the nosebleed is the first emergency treatment, if the nosebleed does not stop and continues to occur frequently or occurs frequently, call the regular pediatrician or hospital emergency room and follow their instructions.
- If a child who has had a lot of nosebleeds at least once in the past or who has had a persistent nosebleed has suffered a nose bleeding and continues to bleed after a nose bleeding, call a medical paramedic, hospital emergency department, or a regular pediatrics department as an emergency
- Treat according to their instructions.
- Most children with allergic rhinitis may bleed more frequently.
- It is common for allergic rhinitis to be less bleeding with proper treatment.
- With allergic rhinitis or other types of rhinitis, snotty may develop more often on the nasal mucosa, and the snotty may stick to the nasal mucosa for a long time.
- The capillaries in the nasal mucosa are stimulated by the snotty, causing the capillaries to burst, causing frequent nosebleeds.
- At this time, according to the doctor’s prescription, apply Bactroban ointment/mupirocin ointment antibiotic ointment or bacitracin antibiotic ointment or cream to the nasal mucosa 3 times a day for 10 days may stop nasal bleeding.
- If the room temperature is above normal, the humidity is very low, and the nasal mucosa layer is dry, you may bleed more frequently. In this case, the room temperature and humidity must be properly adjusted.
- If nosebleeds occur frequently or continue to bleed, parents should provide first aid at home, followed by follow-up treatment by a doctor.
- Sometimes, a part of the capillaries in the nasal mucosa is treated with silver nitrate sticks. Putting a few drops of adrenaline on a cotton ball and putting it in the nasal cavity for a while and then removing it can stop bleeding (adrenaline is a vasoconstrictor drug).
- Nosebleeds from thrombocytopenia, leukemia or several other causes are treated depending on the cause.
- [Parents should also be at least the half-doctors-Pediatric and Family Nursing Encyclopedia]-Refer to Volume 18, Children’s and Adolescent Otolaryngology Diseases-Nonbleeding
The following is an example of the Internet pediatric and adolescent health counseling question and answer on “I have frequent nosebleeds…”.
Q&A.
My boy has frequent nosebleeds...
Q.
- This is a 7-year-old boy. Since childhood, he has been visiting the hospital with a cold.
- From the age of five, he has been moving from pediatrics and adolescents to otolaryngology.
- I know that I have rhinitis and my nose is weak, so I can bleed my nose.
- But it flows too often (once a month).
- Compared to other children. (I’ve never had a nosebleed since I was born…)
- If I was a little bit sick, I wouldn’t have much to worry about. This is really a nosebleed, so you don’t know if it is a nosebleed.
- The hospital says it’s not a big deal, but I don’t bleed nose bleeding when there’s something wrong with my nose. At children’s houses, it only spills little by little. But, oddly enough, when I go to sleep and say’ Mom or my nosebleed’, it sheds a lot. Are they really bleeding noses more often than other children because of rhinitis???
A.
- Dear Seungwon Hello.
- Thanks for asking. Ideally, diagnosis and treatment should be performed by synthesizing the results of the child’s age and gender, past and present family medical history, symptom signs and medical examination findings, and appropriate clinical examinations, but we will respond with the information given in consideration.
- If you are bringing your child to my Pediatrics and Adolescents Department, I will check the past family history, allergy history, growth and development process, pregnancy birth history, habits, and more detailed medical history, and perform a physical examination from head to toe. In particular, let’s look into the nasal cavity with a parenteral or nasal endoscope.
- On physical examination, there are no bleeding spots on the skin, there is no abnormality in the nasal cavity, the nasal mucosa layer is pale, there is an allergic shiner under the eyes, and there is a history of asthma or allergic rhinitis in the past, and it is also an allergic disease to reborn parents. If you have a family medical history, you will be diagnosed as having the most likely nosebleeds from allergic rhinitis. Sometimes allergic rhinitis and sinusitis are common.
- If the result of the physical examination is normal and the parents are worried about the child’s nosebleed and come to consult my pediatrics three or more times, a CBC blood test, a bleeding screening test to determine the cause of bleeding (Table 23 ) to see if there is a systemic hemorrhagic disease.
- These tests are relatively simple blood tests and are tested to see if blood clots well. If the test result is normal, send it to the otolaryngologist
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
-
여러 종류의 지혈 방법 참조
-
외(부)출혈과 내(부)출혈 참조
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
소아가정간호백과-부모도 반의사가 되어야 한다, 이상원 저
-
The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
-
Preparation for Birth. Berverly Savage and Dianna Smith
-
임신에서 신생아 돌보기까지. 이상원
-
Breastfeeding. by Ruth Lawrence and Robert Lawrence
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th-31st Ed 2021
-
Nelson Text Book of Pediatrics 19th-21st Edition
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gerhon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
Growth and Development of Children, George H. Lowrey 8th edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”