전염성 농가진(감염성 농가진). Impetigo contagiosa
(You may visit www.drleepediatrics.com – Chapter 7, Pediatric Adolescent Infectious Diseases or 제 7권, 소아 청소년 감염병 질환 웹사이트)
- 황색 포도상구균 및, 또는 A군 베타 용혈성 연쇄상구균 감염으로 생긴 화농성 피부염을 전염성 농가진, 또는 부스럼이라고 한다.
- A군 베타 용혈성 연쇄상구균,
- 황색 포도상구균, [부모도 반의사가 되어야 한다-소아가정간호백과]-제10권 소아청소년 신장 비뇨 생식계 질환-급성 사구체 신염, 제17권 소아청소년 피부 질환-농가진 참조, 제21권 소아청소년 가정 학교 간호- 배시트라신 연고 참조.
전염성 농가진의 원인
- 불결한 피부, 곤충 물림, 긁힌 상처, 또는 그 외 다른 상처 등으로 생긴 피부 상처에 황색 포도상구균 및, 또는 A군 베타 용혈성 연쇄상구균이 감염될 때 전염성 농가진이 생길 수 있다.
- 농가진은 모든 연령층 아이들에게 생길 수 있지만 신생아들과 영유아들에게 더 잘 생길 수 있다.
- 사시사철 어느 계절에도 전염성 농가진이 생길 수 있지만 여름철에 더 잘 생긴다.
- 잠복기는 7~10일이다.

사진 241. 얼굴 특히 입술주위에 난 A군 베타 용혈성 연쇄상구균성 전염성 농가진.
Copyright ⓒ 2013 John Sangwon Lee, M.D.. FAAP

사진 242. 얼굴에 난 전염성 농가진, 특히 턱에 A군 베타 용혈성 연쇄상구균성 농가진이 날 수 있다.
Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP

사진 243. 팔과 몸통에 난 A군 베타 용혈성 연쇄상구균 감염으로 생긴 전염성 농가진
팔에 생긴 농가진이 접촉 된 몸통 부위에도 농가진이 생겼다.
Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP

사진 244. 왼쪽 팔에 난 전염성 농가진이 황색 포도상구균 농가진.
Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP

사진 246. 발등에 난 A군 베타용혈성 연쇄상구균 감염으로 생긴 전염성 농가진.
Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP

사진247. 콧구멍과 그 주위에 난 황색 포도상구균 전 염성 농가진.
Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP

사진 245. 양쪽 앞 팔에 난 황색 포도상구균 전염성 농가진.
Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
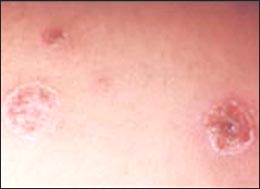
사진 248. 배에 난 황색 포도상구균 전염성 농가진.
Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
전염성 농가진의 증상 징후
- 농가진을 일으킨 황색 포도상구균 및, 또는 A군 베타 용혈성 연쇄상구균의 종류, 전염성 농가진의 정도, 환아의 나이, 합병증의 유무 등에 따라 증상 징후가 다르다.
- 농가진은 얼굴, 목, 몸통, 엉덩이, 겨드랑이, 팔, 다리 등에 주로 난다. 전염성 농가진이 처음 시작할 때 피부가 불거지고, 맑은 물집이 잡힌 소수포가 생긴다.
- 그 물집에 고름이 잡히고 농포가 생기고
- 농포가 터지고 마른 딱지(가피)가 생기는 것이 자연 진행 과정이다.
- 농포 속에 있는 황색 포도상구균이나 A군 베타 용혈성 연쇄상구균이 환아의 다른 피부로 계속 번질 수 있고
- 농가진에 접촉된 다른 사람의 피부에도 농가진이 생길 수 있다.
- 농가진의 크기와 모양은 다양하다.
- 그 직경은 수mm~4cm 정도 크고 그 모양은 둥글둥글하기도 하고 일정한 모양이 없이 다양하다.
- 농가진의 가장자리는 붉고 중앙부는 꿀 색 비슷한 딱지로 덮여 있기도 하고 전염성 농가진에서 고름이 날 수 있다.
- 전염성 농가진이 나으면 전염성 농가진이 나 있었던 피부는 정상 피부로 돌아간다.
- 농가진으로 가려워 긁으면 딱지가 떨어지면서 피고름이 날 수 있고 그 피고름 속에 있는 박테리아가 다른 부위로 퍼질 수 있다.
- A군 베타 용혈성 연쇄상구균 감염으로 생긴 전염성 농가진의 주위에 있는 림프절이 부을 수 있다.
전염성 농가진의 진단
- 증상, 징후, 진찰 소견, 전염성 농가진 환부에서 채취한 고름, 딱지 등 피검 물로 세균 배양 검사 등으로 진단할 수 있지만 세균 배양 검사를 하지 않고 증상, 징후, 시진으로 진단하는 경우가 더 많다.
전염성 농가진의 치료
- 농가진을 일으킨 A군 베타 용혈성 연쇄상구균의 특정 균종의 항원 항체 반응으로 급성 사구체 신염이 생길 수 있고,
- A군 베타 용혈성 연쇄상구균이 골수에 감염되어 골수염 등이 생길 수 있다.
- 농가진 환부에 직접 접촉되면 본인이나 다른 사람들에게 쉽게 전염될 수 있다.
- 이런 저런 이유로 전염성 농가진은 조속히 치료해야 한다.
- 다 나을 때까지 1회용 밴드 에이드나 거즈 등으로 전염성 농가진 병소를 덮어 더 이상 전염되지 않게 예방한다.
- 합병증이 없고 몇 개 정도 난 전염성 농가진은 Mupirocin 연고(박트로반 항생제 연고, Bactroban ointment), Bacitracin 연고, Bacitracin-polymixin B 연고를 7~10일간 환부에 발라 치료하면 잘 낫는다.
- 합병증이 있거나 여러 군데에 많이 난 전염성 농가진이나 자주 재발하는 전염성 농가진은 경구용 Dicloxacillin, Oxacillin, Cloxacillin, 또는 1세대 Cephalosporins 계 항생제들 중 Cephalexin으로 치료하고 Bactroban(Mupirocin)연고나 Centany(Mupirocin) 연고로 치료할 수 있다.
- Amoxicillin-clavulanate potassium 등 경구용 항생제로 치료한다.
- 봉화직염(봉소염)이나 신체 내장에 생긴 합병증은 병원 입원 혈관 항생제로 치료한다.
- 메티실린 내성 포도상구균(MRSA) 감염에 의한 포도상 구균 농가진의 발생률이 증가 일로에 있다.
- 이상 열거한 항생제로 치료 되지 않으면 메티실린 내성 포도상구균 감염에 의한 농가진인가 의심하고 Clindamycin이나 Vancomycin 등의 항생제로 치료한다.
출처 및 참조문헌
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.243
전염성 농가진의 합병증
- 농가진을 하찮은 부스럼 병으로 생각해서는 안 된다.
- 전염성 농가진을 일으킨 A군 베타 용혈성 연쇄상구균이나 황색 포도상구균은 신체 다른 부위로 감염될 수 있고 종기, 림프절염, 골수염, 관절염, 폐렴, 패혈증 등 합병증을 일으킬 수 있다.
- 또 A군 베타 용혈성 연쇄상구균의 여러 균종들 중 급성 사구체 신염을 일으킬 수 있는 특정 균종이 있다.
- 이 균종에 감염되어 생긴 전염성 농가진을 적절히 조속히 치료해주지 않으면 급성 사구체 신염이 생길 수 있다.
- 때로는 적절히 조속히 치료해도 급성 사구체 신염을 완전히 예방할 수 없다.
- 메티실린 내성 포도상구균(MRSA) 감염에 의한 포도상 구균 농가진의 발생률이 증가 일로에 있고 치료 상 문제가 많이 생길 수 있다.
Infectious impetigo (infectious impetigo)
Purulent dermatitis resulting from Staphylococcus aureus and or group A beta-hemolytic streptococcal infection is called infectious impetigo.
Group A beta-hemolytic streptococcus, Staphylococcus aureus, [Parents should also be at least half doctors-Encyclopedia of Pediatrics and Family Nursing]-Volume 10 Child and adolescent kidney urogenital disease-Acute glomerulonephritis, Volume 17 Child and adolescent skin diseases-Refer to impetigo, Vol.21 Pediatric Family School Nursing- See Bacitracin Ointment. Causes of infectious impetigo can occur when Staphylococcus aureus and or group A beta-hemolytic streptococci are infected with skin wounds resulting from unclean skin, insect bites, scratches, or other wounds. Impetigo can occur in children of all ages, but it can be more prevalent in newborns and infants.
Contagious impetigo can develop in any season of the year, but it is more common in summer.
The incubation period is 7-10 days.
Photo 241. Group A beta-hemolytic streptococcal infectious impetigo on the face, especially around the lips. Copyright ⓒ 2013 John Sangwon Lee, M.D. FAAP
Photo 242. Infectious impetigo on the face, especially group A beta-hemolytic streptococcal impetigo on the chin may occur. Copyright ⓒ 2013 John Sangwon Lee, M.D., FAAP
Picture 243. Infectious impetigo resulting from group A beta-hemolytic streptococcal infection on arms and trunk. Impetigo was also formed on the part of the body where the impetigo on the arm was in contact. Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
Picture 244. Staphylococcus aureus impetigo is infectious impetigo on the left arm. Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
Picture 246. Infectious impetigo resulting from group A beta-hemolytic streptococcal infection on the instep. Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
Picture 247. Staphylococcus aureus infectious impetigo in the nostrils and around it. Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
Picture 245. Staphylococcus aureus contagious impetigo on both forearms. Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
Picture 248. Staphylococcus aureus infectious impetigo in the stomach. Copyright ⓒ 2012 John Sangwon Lee, M.D., FAAP
Symptoms, signs of infectious impetigo
Symptoms differ depending on the type of Staphylococcus aureus causing impetigo, or group A beta-hemolytic streptococcus, the degree of infectious impetigo, the age of the patient, and the presence or absence of complications.
Impetigo occurs mainly on the face, neck, torso, buttocks, armpits, arms, and legs.
When the first infectious impetigo begins, the skin bulges, and vesicles with clear blisters develop.
The blisters get pus and pustules.
Pustules burst and dry scabs (crusts) appear as a natural process. Staphylococcus aureus or group A beta-hemolytic streptococcus in the pustules may continue to spread to the patient’s other skin.
Impetigo can also develop on the skin of other people in contact with impetigo.
Impetigos vary in size and shape.
Its diameter is about several mm~4cm, and its shape is round and there is no regular shape.
The edges of the impetigo are red, and the central part is covered with a honey-like scab, and pus may be produced from the infectious impetigo.
When infectious impetigo is healed, the skin that had infectious impetigo will return to normal skin.
Scratching itchy with impetigo can cause the scab to fall, causing blood pus, and the bacteria in the blood pus can spread to other areas.
The lymph nodes around the infectious impetigo resulting from group A beta-hemolytic streptococcal infection may swell.
Diagnosis of infectious impetigo
Symptoms, signs, examination findings, pus, and scabs collected from infectious impetigo can be diagnosed by bacterial culture tests, but more often diagnosed by symptoms, signs, and examination without bacterial culture tests.
Treatment of infectious impetigo
Acute glomerulonephritis may occur due to an antigen-antibody reaction of a specific strain of group A beta-hemolytic streptococcus which caused impetigo, Group A beta-hemolytic streptococcus can infect the bone marrow, resulting in osteomyelitis.
Direct contact with impetigo-affected areas can be easily transmitted to himself or others.
For one reason or another, infectious impetigo should be treated promptly. Cover the infectious impetigo lesion with a disposable band-aid or gauze until it is healed to prevent further contagion.
A few infectious impetigos without complications can be cured by applying Mupirocin ointment (Bactroban ointment), Bacitracin ointment, and Bacitracin-polymixin B ointment to the affected area for 7 to 10 days.
Infectious impetigo that has complications or occurs frequently in several places, or frequently recurring infectious impetigo, can be treated with oral Dicloxacillin, Oxacillin, Cloxacillin, or Cephalosporins, among the first-generation antibiotics, with Cephalexin and Bactroban (Mupirocin) ointment have.
It is treated with oral antibiotics such as amoxicillin-clavulanate potassium.
Cellulitis or complications in the body’s internal organs are treated with vascular antibiotics hospitalized.
The incidence of staphylococcal impetigo caused by methicillin-resistant staphylococcus aureus (MRSA) infection is on the rise.
If it is not treated with the antibiotics listed above, it is suspected that it is impetigo caused by a methicillin-resistant staphylococcal infection and treated with antibiotics such as Clindamycin or Vancomycin. Sources and references The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, Complications of infectious impetigo Impetigo should not be considered a petty swelling disease.
Group A beta-hemolytic streptococcus or Staphylococcus aureus, which causes infectious impetigo, can infect other parts of the body and cause complications such as boils, lymphadenitis, osteomyelitis, arthritis, pneumonia, and sepsis.
In addition, among the several bacterial species of group A beta-hemolytic streptococcus, a specific species can cause acute glomerulonephritis.
Acute glomerulonephritis can occur if infectious impetigo resulting from infection with this fungus is not treated properly and promptly. Sometimes acute glomerulonephritis cannot be completely prevented even with prompt and adequate treatment.
The incidence of staphylococcal impetigo caused by methicillin-resistant staphylococcus aureus (MRSA) infection is on the rise, and treatment problems can arise.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Nelson Textbook of Pediatrics 14th ed. Beherman,
-
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th edition 2012
-
Nelson Text Book of Pediatrics 19th Edition
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 안효섭 외 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”