요로 감염 Urinary tract infections(UTI)
요로 감염과 용어
- 요로 Urinary tract–신장·요관·방광·요도를 통틀어 비뇨기계, 비뇨기계통, 비뇨기 또는 요로라고 한다.
- 신장염 Nephritis–박테리아 감염이나 바이러스 감염 등 병원체 감염이 신장에만 생긴 감염병을 신장염이라한다.
- 신우신염 Pyelonephritis–박테리아 감염이나 바이러스 감염 등 병원체 감염이 신장과 신우에 동시 감염됐을 때를 신우신염이라 한다.
- 방광염 Cystitis–박테리아 감염이나 바이러스 감염 등 병원체 감염이 방광에만 생긴 감염병을 방광염이라 한다.
- 요도염 Urethritis–박테리아 감염이나 바이러스 감염 등의 병원체 감염이 요도에만 생긴 감염병을 요도염이라 한다.
- 요로 감염 Urinary tract infections–전체 요로(신장, 요관, 방광, 요도)에 생긴 감염병을 요로 감염이라고 진단하기도 하고, 요로의 일부에만 생긴 감염병을 요로 감염이라고 진단하기도 한다.
- 무증상 요로 감염–요로 감염병은 있지만 증상이 없으면 무증상 요로 감염(Asymtomatic urinary tract infections)이라 한다. 사실은, 무증상이 아니라 증상 징후가 있지만 요로 감염병이 있는지 모르고 지내고 있는 요로 감염병이라고 할 수 있다.
소아청소년의 비뇨기계 해부와 요로 감염(그림 1-36)
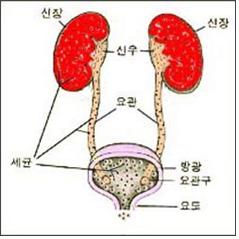
그림 1-36. 신장, 요관, 방광과 요도를 요로라고 한다. 요로의 일부나 전체에 생긴 감염을 요로 감염이라 한다.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
-
특히 영유아의 경우, 신장에서부터 방광까지의 거리와 신장에서 요도의 외요도까지 거리가 성인 것에 비해 아주 짧고, 영유아들은 박테리아나 바이러스 등 병원체의 감염에 저항할 수 있는 감염병 방어 면역체계 기능이 미약하며, 그 외 다른 여러 가지 이유로 특히 영유아들은 요로 감염에 더 잘 걸린다.
-
게다가 비뇨기계에 선천성 기형 또는 후천성 이상 등으로 영유아들에게 요로 감염이 더 잘 생길 수 있다.
-
영유아의 요로에 박테리아 감염이 생기면, 박테리아가 신장·방광·요관·요도 중 일부의 요로 부분에만 국한되어 감염되지 않고, 신장의 실질에서 신우·요관·방광·요도까지, 또는 요도에서 신장의 실질까지 전체 요로가 동시 감염되는 요로 감염병이 생기는 것이 보통이다.
-
마치 감기가 걸릴 때 비강에만 바이러스 감염이 생기지 않은 비강, 부비강, 인두 강, 아데노이드, 편도 전체가 감염되듯이, 어린 영유아들의 요로가 박테리아에 감염되면 박테리아 신장염, 박테리아 신우염, 박테리아 방광염, 박테리아 요도염 등이 따로따로 생기는 경우는 흔치 않다.
요로 감염 발생률
-
생후 1~4일의 신생아 : 1%
-
영아 : 2%
-
학령기 여아 : 1.1%
-
젊은 여성 : 1%
-
임신한 여성 : 5%
-
60세 이상의 남성 : 1.6% , 출처 : David Scheifele, M.D
요로 감염의 원인
- 소아청소년(0~18세)에게 생기는 급성 요로 감염은 소아청소년에게서 흔히 볼 수 있는 전체 급성 감염병 중 하나이다.
- 1세 이전 남아의 3.3%, 여아의 6.5%가 급성 요로 감염에 걸린다.21(참고; 위 정보와 다른 점).
- 소아청소년 요로 감염의 30~40%에서 방광 요관 역류가 발견된다.
- 방광 요관 역류로 생긴 소아청소년 요로 감염을 적절히 치료하지 않으면, 요로 감염이 재발될 수 있고 고혈압, 신장손상과 신장 상흔 등 후유증이 생길 수 있다21.
소아청소년 요로 감염을 일으킬 수 있는 병원균과 감염경로
-
대장균(E. coli)이 80%이고,
-
나머지는 클렙시엘라균 (Klebsiella) ,
-
엔테로박터속균(Enterobacter)
-
연쇄상구균(Streptococci),
-
프로테우스균(Proteus),
-
슈도모나스균(Sudomonas),
-
장구균(Enterococci ), 세라티아속균(Serratia), 헤랄리아속균, 황색 포도상구균(Staphyloccocus Aureus) 등 세균이 요로감염을 더 흔히 일으킬 수 있다.
-
여러 종류의 박테리아 중 한 종류의 박테리아 감염 또는 한 종류 이상 여러 종류의의 박테리아가 요도 입구에 감염된 후→ 그 박테리아가 요도→방광→요관→신장 등의 순서로 전체 요로에 감염되어 요로 감염을 일으키는 경우가 가장 흔한 감염 경로이다.
-
드물게는, 캔디다 진균 감염에 의해서도 요로 감염이 생길 수 있다.
-
비뇨기계 이외 다른 신체 계통의 기관이나 조직의 감염병을 일으켰던 박테리아 등 병원체나 패혈증을 일으킨 박테리아 등 병원체가 혈류를 따라 신장에 2차 감염을 일으키고 그로 인해 신우 신염을 일으킬 수 있다.
-
신우신염을 일으킨 박테리아가 신장 신우에서→요관→방광→요도의 순서로 계속 퍼져 전체 요로에 감염될 수 있다.
-
여아의 외 요도구와 항문 사이의 거리가 남아에 비해 해부학적으로 훨씬 더 짧고 정상적 위생 관리 문제, 외음부와 비뇨기의 특이한 해부학적 구조로 인해, 대변에 있는 위장관 대장균이 의해 외 요도구에 감염되어 여아들은 남아들보다 요로 감염에 더 쉽게, 더 자주 걸릴 수 있다.
-
대변을 본 후 항문 쪽에서 외음부 쪽으로 항문을 닦는 버릇이 있거나, 특히, 여 영유아들은 요로 감염에 더 잘 걸릴 수 있다.
-
남녀 신생아들에게 생기는 요로 감염의 발생 빈도와 1세 이전 남녀 영아들에게 생기는 요로 감염의 발생 빈도는 거의 비슷하지만, 첫 돌 이후 여 유아들의 요로 감염 발생 빈도는 남 유아들의 요로 감염 빈도보다 훨씬 더 높다.
-
이중 요관, 요관류나, 게실, 후부 요도 판막증, 방광 요관 폐쇄증 등 신장·요관·방광, 또는 요도 등에 생긴 선천성 비뇨기계 기형이 있거나, 선천성 신경성 방광 또는 후천성 신경성 방광이나 근육의 이상 등이 있으면 요로 감염에 더 잘 걸릴 수 있다.
표 1-3. 나이에 따른 요로 감염의 증상 징후(%)
| 요로감염의 징후증상 | 생후부터 1개월 까지 | 생후 1개월~ 2세 | 2~5세 | 5~12세 |
| 성장 장애와 성장 지연, 음식물 섭취문제 | 53% | 36% | 7% | – |
| 과민, 산통(콜이크) | – | 13% | 5% | – |
| 소변에서 냄새가 난다, 소변이 혼탁 | – | 8% | 14% | – |
| 설사 | 18% | 16% | – | – |
| 구토 | 25% | 29% | 16% | 3% |
| 열 | 11% | 38% | 57% | 50% |
| 경련 | 2% | 6% | 9% | 5% |
| 혈뇨 | – | 6% | 16% | 6% |
| 빈뇨, 배뇨곤란 | – | 4% | 34% | 40% |
| 야뇨증 | – | – | 27% | 29% |
| 복통 | – | – | 23% | 44% |
| 옆구리 통증 | – | – | – | 12% |
출처: RiILeY H.D. Pyelonephritis in children, Hospital practice 3, 1972.
요로 감염의 증상 징후
-
요로 감염의 중증도, 요로 감염 발생 전 선행병, 급성 요로 감염 또는 만성 요로 감염, 환아의 나이(일령, 월령, 연령 등), 요로 감염을 일으킨 박테리아의 종류, 선천성 요로 기형의 유무 및 그 종류와 정도 등에 따라 요로 감염의 증상 징후가 많이 다르다.
-
신생아, 영아, 유아가 급성 요로감염 또는 만성 요로 감염을 앓을 때 열, 배뇨 곤란, 소변 자주 보기, 혈뇨, 뿌연 색 소변, 악취 나는 소변, 밤낮을 가리지 않고 오줌 싸기, 아랫배 아프기 또는 옆구리 아프기 등의 증상 징후가 나타날 수 있다.
-
그 외 다음과 같은 다양한 증상 징후가 요로 감염으로 생길 수 있다.
-
별다른 이유 없이 잘 먹지 않고, 보채고, 미열 내지 고열이 갑자기 나기도 하고, 그런 열이 며칠 동안 나다가 더 이상 나지 않을 수 있고, 하루에도 얼마 동안 열이 나다가 안 나기도 하며, 체중이 정상적으로 늘지 않고, 또래보다 잘 크지 않을 수 있다.
-
때로는 고열·구토·복통·설사·경기 등 비뇨기계통 질환에서 나타나는 일반적인 증상 징후와는 별로 관련이 없는 증상 징후가 갑자기 생길 수 있다.
-
요로 감염을 앓는 아이의 소변을 검사해 보지 않고서는 요로 감염에 걸려 있는지 확실히 알 수 없는 때도 많다.
-
특히 영유아가 요로 감염을 앓고 있는지 잘 모르고 위장염·감기·중이염 또는 독감 등을 앓고 있다고 오진하고 항생제로 치료하는 때도 간혹 있다.
-
요로 감염에 걸린 2~3세 여아들 중 일부는 소변을 가릴 수 있는 나이에 소변을 가리지 못하고 옷에 오줌을 질금질금 밤낮 가리지 않고 싸기도 한다.
-
요로 감염에 걸린 일부의 영유아들 중 외음부가 빨갛게 발적될 수 있고, 소변에서 고약한 냄새가 날 수 있다.
-
학령기 아이가 요로 감염에 걸리면 소변을 자주 보고, 소변을 봐도 개운치 않고, 아랫배가 아프다고 호소할 수 있다.
-
소변을 볼 때 아파서 소변을 잘 볼 수 없는 경우도 있고, 아랫배가 팽만할 수 있다.
-
며칠 동안 고열이 계속 나면서 한쪽 옆구리나 양쪽 옆구리가 아플 수 있다.
-
소변에 피가 빨갛게 섞여 나올 수 있고, 피가 극소량 나올 때도 있다.
-
소변 현미경 세균 검사를 해 보면, 소변에 세균이 있는지 알 수 있고, 멀티스틱스 소변 화학 검사를 해 보면 피가 소변에 있는 것을 알 수 있다.
-
이와 같이 요로 감염이 있을 때, 때로는 소변에 피가 있는지 육안으로는 볼 수 없고, 현미경 검사로 소변의 피를 볼 수 있다. 또 요로 감염이 있으면 육안으로 볼 수 있을 정도로 소량의 피가 소변에 나올 수 있고, 때로는 육안으로 볼 수 있을 정도로 빨간 피가 소변에 나올 수도 있다.
-
소변에 백혈구가 많이 나와서, 소변 색이 뿌옇게 변할 수 있다.
-
급성 요로 감염을 바로 적절히 치료하지 않으면, 급성 요로 감염이 만성 요로 감염으로 이어질 수 있다.
-
요로 감염을 조기에 적절히 치료하지 않으면, 급성 요로 감염이 만성 신우신염이 될 수 있고, 혈압이 비정상적으로 높아져 2차 고혈압이 생길 수 있고 빈혈도 생길 수 있다.
-
만성 신우신염을 적절히 치료하지 않으면, 신장의 일부나 전체가 일시적으로 또는 영구적으로 손상될 수 있고, 손상된 신장 전체를 수술로 떼어내야만 요로 감염이 완치되는 경우도 있다.
요로 감염의 진단

사진 1-37. 멸균 컵에 피검물용 소변을 받아 소변 화학 검사, 소변 현미경 세균 검사, 소변 세균 배양 검사와 항생제 감수성 검사를 한다.
Copyrightⓒ 2011 John Sangwon Lee,MD.FAAP
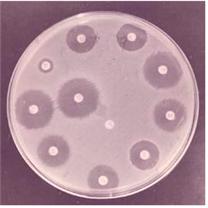
사진 1-38. 소변으로 소변 세균 배양 검사를 할 수 있다. 자란 세균으로 세균 항생제 감수성 검사를 한다. 세균 항생제 감수 검사에서 얻은 결과에 따라 가장 효과 있는 항생제로 요로 감염을 치료하는 것이 이상적 치료이다.
Copyrightⓒ 2011 John Sangwon Lee,MD.FAAP
-
병력, 증상 징후와 진찰소견 등을 종합하여 요로 감염이 있다고 의심되면, 멀티스틱스 소변 화학 검사, 현미경 소변검사와 소변 세균 배양 검사 등으로 진단하는 것이 보통이다.
-
소변 세균 배양 검사용 소변은 깨끗한 멸균 컵에 받아야 한다.
-
가능한 한 소변 세균 배양 검사를 해서 요로 감염을 일으킨 박테리아의 종류가 무엇인지 알아내고, 세균 항생제 감수성 검사를 해서 그 검사 결과에 따라 가장 적절한 항생제를 선택하여 치료하는 것이 이상적이다.
-
요로 감염이 급성인지 또는 만성인지 요로 감염에 걸린 환아의 나이, 요로 감염을 일으킨 선행 이상이나 질병에 따라 진단 방법이 다르다.
-
2세 이전 영유아에게 급성 요로 감염이 생기면,
-
신장 초음파 검사와
-
배뇨 방관 요도 조영술(Voiding cystourethrography/VCUG) 검사
-
또는 방사핵종 방관 요도 조영술 검사를 기본적으로 하여 요로 감염을 진단하고 요로에 어떤 이상이 있는지 알아볼 것을 권장한다.
-
신장 초음파 검사로 수신증이 있는지, 다른 종류의 신장 해부 이상이나 기형이 있는지 알아볼 수는 있지만, 신장 초음파 검사는 방광 요관 역류가 있는지 알아보는 데에는 부적절한 검사이다.
-
DMSA 신장 스캔 검사로 신장의 어느 부위가 어느 정도로 손상되어 있는지 알아볼 수 있다.
-
정맥 내 신우 촬영술(IVP)은 요즘 많이 쓰지 않는 검사이다.
-
아주 드물게는, 필요에 따라 비뇨기과 전문의가 특수 거울이 달린 방광경을 요도관을 통해 방광 속에 넣고 방광경을 통해 요도와 방광 속을 육안으로 직접 보고 요관류, 게실, 후부 요도 판막증, 방광 요관의 폐쇄증 등이 있는지 진단·치료하기도 한다.
-
소변 화학 검사와 현미경 소변 검사를 한 번 해서 요로 감염을 확진할 수 없는 때도 가끔 있다. 따라서 소변 화학 검사와 현미경 소변 검사를 두세 번 반복해서 요로 감염을 확진하기도 한다.
표 1-4. 나이에 따른 세균뇨(Bacteriuria) %
| 나이(월령 또는, 세) | 발생 율(%) | 남아 여아 발생 비율 |
| 생후부터 1개월까지(신생아들) | 1% | 1.5(남아) : 1(여아) |
| 생후 1개월 ~2세(영아들과 유아들) | 2% | 1.5(여아) : 1(남아) |
| 2~5세(유아와 학령기 이전아이들) | 1~2% | 4.8(여아) : 1(남아) |
| 5~16세(학령기 아이들과 사춘기 아이들) | 1~2%(여아) 0.05%(남아) | 1.5(남아) : 1(여아) |
출처와 참조문헌 D. Heller’s lecture at Havard Medical School
세균뇨 (Bacteriuria) 참조
소아청소년의 첫 번째 요로 감염과 배뇨 방광 요도 조영술(VCUG) 검사
-
요로에 선행 이상이나 질병이 전혀 없는데 요로 감염이 생길 수 있다.
-
그러나 요로에 어떤 선천성 기형 또는 후천성 기형 등 선행 이상이 있을 때에는 요로 감염이 더 잘 생길 수 있다.
-
초음파 검사로 신장의 크기나 방광 요관 역류 유무 등을 검사할 수 있다. 그러나 때로는 정확한 검사결과가 나오지 않을 수 있다.
-
소아청소년에게 최초 요로 감염이 생겼을 때, 배뇨 방광 요도 촬영 검사를 꼭 해야 하는지 또 하지 한해도 되는지 의학계 논쟁거리다. 그러나 요즘 통상적으로 그 검사를 하라고 권장한다.
-
배뇨 방광 요도 촬영 검사를 하면 방광 요관 역류가 있는지 없는지 확실히 알아낼 수 있다.
-
신장이 부어 있는지, 신장에 상처, 상흔, 또는 수신증이 있는지, 신장의 크기가 정상인지, 또 방광 요관 역류가 있는지 알아보는 데 배뇨 방광 요도 조영술 검사 결과보다 신장 초음파 검사 결과가 더 신빙성이 있다.
-
따라서 소아청소년에게 최초 요로 감염이 생겼을 때에는 배뇨 방광 요도 조영술 검사와 신장 요관 방광 초음파 검사 등을 해보는 것이 좋다.
-
어떤 종류의 검사를 할 것인지, 어느 정도까지 할 것인지 등은 담당 의사의 판단에 따라야 한다(방광 요관 역류 참조).

사진 1-39. 정맥 내 신우 촬영술 검사 사진.
a-좌우 신장, b, c-좌우 요관.
Copyrightⓒ 2011 John Sangwon Lee,MD.FAAP
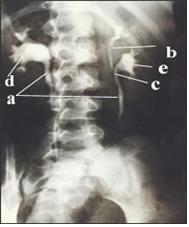
사진 1-40. 정맥 내 신우 촬영술 검사사진. a-좌우 요관, b-이중 요관 중 상 이중 요관, c-이중 요관 중 하 이중 요관, d-우 신장, e-좌 신장.
Copyrightⓒ 2011 John Sangwon Lee,MD.FAAP

사진 1-42. 배뇨 방광 요도 조영술 검사 사진 – 좌 신우에 소변이 비정상적으로 많이 차 있고 그쪽 신장이 손상되어 있다.
a-손상된 신장, b-정상 방광.
Copyrightⓒ 2011 John Sangwon Lee,MD., FAAP
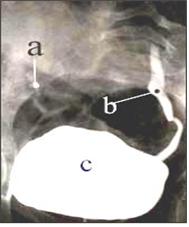
사진 1-41. 배뇨 방관 요도 조영술 사진.
좌 요관이 비정상적으로 확장되어 있다.
a-우 요관, b-좌 요관, c-방광.
Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
요로 감염의 치료 및 예방
- 요로 감염의 증상 징후와 정도, 선천성 요로 기형의 유무, 원인, 합병증의 유무 등에 따라 치료가 다르다.
- 영유아나 학령기 아이가 급성 요로 감염으로 고열이 나면서 심하게 앓으면 병원에 입원해서 적절한 항생제 혈관주사로 치료하는 것이 보통이다.
- 소아청소년 급성 요로 감염을 경구용 항생제로 적절히 치료한 결과와, 적절한 혈관주사 항생제로 치료한 결과와 거의 같다는 연구가 있다. 그래서 최근에는 경구용 항생제로 급성 요로 감염을 치료하는 경향이 있다 2.
- 열도 없고 별다른 증상이 없는 요로 감염은 의사의 처방에 따라 아목사실린이나 박트림 또는 그 외 적절한 항생제로 10일 간 치료하기도 한다.
- 요로 감염에 처음 걸린 아이나, 과거에 단 한 번이라도 요로 감염을 앓았던 과거 병력이 있는 아이의 경우, 신장, 요도, 방광 초음파 검사, 배뇨 방광 요도 조영술 검사 또는 정맥 내 신우 촬영술 검사 등으로 신장·요관·방광·요도가 정상인지 알아보는 것이 좋다.
- 요로 감염에 두 번 이상 걸린 소아청소년들의 상당수가 선천성 요로 기형이 있거나, 어떤 후천성 이상 등 요로에 선행 이상이 있는 것을 발견할 수 있기 때문이다.
- 첫 돌 이후 요로 감염에 걸린 남아들의 대부분은 요로에 선천성 기형이 있을 가능성이 많다. 따라서 첫 돌 후 남아가 요로 감염에 걸리면 요로에 선천성 기형이 있는지 알아보기 위해 신장·요관·방광 등의 요로 초음파 검사, 정맥 내 신우 촬영술, 신장 X-선 사진, CT 스캔 검사 등으로 전체 비뇨기계 검사를 권장한다.
- 과거 한 번 요로 감염을 앓았던 아이에는 요로 감염에 자주 걸일 수 있다. 그래서 소변 화학 검사, 현미경 소변 검사와 소변 세균 배양 검사 등을 정기적으로 추적 검사하는 것이 좋다.
- 요로 감염이 자주 재발할 때에는, 원인이 되는 원래의 선행 감염병을 적절한 항생제로 치료한 후, 나이트로푸란토인(니트로푸란토인/Nitrofurantoin)이나 설파제 등으로 몇 달 내지 몇 년 동안 계속 예방적 치료를 하여 요로 감염 재발을 예방하라고 권장했었다.
- 그러나 최근에는 방광 요관 역류가 있고 요로 감염이 재발해도, 예방적 항생제로 예방적 치료를 꼭 할 필요가 없다는 연구 결과도 있다.
- 방광 요관 역류의 정도가 심하고 요로 감염이 재발하는 병력이 있는 아이의 경우에는, 예방적 항생제 치료를 선택적으로 할 수 있다고 권장한다.
- 나이트로푸란토인 요로 감염 예방적 치료의 효과보다 Cefixime 요로 감염 예방적 치료의 효과가 더 좋고, 반대로 나이트로푸란토인 요로 감염 예방적 치료를 할 때 생기는 부작용이, Cefixime 요로 감염 예방적 치료 할 때의 부작용보다 덜 생긴다22.
- 장기간 소량의 Trimethoim-sulfamethoxazole으로 요로 감염 예방적 치료를 한 결과, 재발성 요로 감염 발병률이 감소됐다는 연구 결과도 있다(출처: NEJM October 29, 20097 p.17490).
- 이상 설명한 바와 같이, 요로 감염의 예방적 치료에는 여러 가지 방법이 있다. 어디까지나, 담당 의사가 그때그때 치료 방법을 적절히 선택해야 한다.
- 경도 방광 요관 역류가 있을 때에는, 항생제로 요로 감염의 예방적 치료를 하면서 2년마다 VCUG 검사를 하고, 중등도 내지 중증도 방광 요관 역류가 있을 때는 3년마다 VCUG 검사를 하는 것을 권장한다.
- 나이트로푸란토인 참조
- 미국 NICE 소아청소년(16세 이하) 요로 감염의 진단·치료·예방에 관한 최신 진단 치료 지침이 나왔지만, 그 지침에 관해 논쟁이 있다(2007년)23.
미국 NICE 소아청소년 요로 감염의 진단, 치료 예방 지침 정보를 소개하면 다음과 같다.
-
생후 3개월 이하의 영아에게 요로 감염이 생기면, 소아청소년 감염과 전문의에게 의뢰하여 혈관 항생제 치료를 받으라고 권장한다. 그러나 3개월 이상 된 영아에게 생긴 신우신염은 경구용 항생제로 7~10일간 치료하라고 권장한다.
-
생후 3 개월 이상 된 영유아에게 방광염이나 하 요로 감염이 생기면, 경구용 항생제로 3일간 치료하라고 권장한다.
-
통상적인 항생제 예방적 치료는 더 이상 권장하지 않는다.
-
방광 요관 역류를 진단하기 위한 통상적 영상 검사를 더 이상 권장하지 않는다.
-
생후 6개월 이상의 영유아에게 생긴 요로 감염을 치료하기 시작해서 치료 효과가 나타나면, 통상적인 초음파 검사를 하지 않아도 된다고 권장한다.
-
그러나 생후 6개월 이하 영아에게 생긴 요로 감염을 치료 시작해서 치료 효과가 나타나지 않으면, 초음파 검사를 6주 내 하라고 권장한다.
-
재발성 요로 감염, 합병증을 동반한 요로 감염 또는 비전형적 요로 감염이 있을 때에는, 급성으로 앓고 있는 중에도 초음파 검사를 하라고 권장한다.
-
생후 3세 이하의 영유아에게 재발성 요로 감염, 합병증을 동반한 요로 감염 또는 비전형적 요로 감염이 있을 때에는, 진단 4~6개월 후에 DMSA 검사를 하라고 권장한다.
- 이와 같이 요로 감염의 진단·치료·예방에 관련된 권장에 관한 정보도 혼동이 생길 수 있다.
- 어디까지나 담당 의사의 지시에 따라 요로 감염을 치료하는 것이 가장 좋다고 생각한다.
요로 감염의 경과
-
전체 요로의 어느 부분도 차단되지 않고 생긴 요로 감염은 거의가 완치될 수 있다.
-
요로에 선천성 기형이 있고 요로 감염이 있을 때는, 내과적 치료와 외과적 치료를 통해 60% 완치될 수 있다.
-
재발성 요로 감염 또는 만성 요로 감염은 장기 추적 치료에서 거의 50%가 완치된다.
-
지속 요로 감염이 22% 생긴다.
-
8%는 신부전증이 생긴다.
(D. Heller의 소아청소년과 연수 교육 강의에서)
요로 감염의 재발
-
-
요로 감염의 80%가 재발된다.
-
매번 적절히 치료 하면 20-25%에서 요로감염이 완화되고, 2년 이 후 재발될 수 있다.
-
성인 여성의 경우, 성교 후 65%가 재발될 수 있다.
(D. Heller의 소아청소년과 연수 교육 강의에서)
-
|
다음은“요로감염과 소변검사”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 요로감염과 소변검사
Q.
- 안녕하세요? 친절한 답변을 해주시는 걸 보고 저도 이렇게 글을 올립니다. 성실한 답변 부탁드립니다.
- 태어난 지 백일이 다 되어 가는 남자 아기에요. 태어나서 황달 땜에 병원입원을 하고 그 후 요로 감염 땜에 일주일 또 입원했어요. 신장 기형아인가 해서 동위원소 검사, 신장, 방광 엑스레이 촬영 등을 했고 세균성 배양검사도 했어요.
- 그런데 약물치료로 일주일 하고 나면 또 며칠 뒤에 곰팡이균, 그 다음에는 또 대장균 등으로 다시 요로 감염을 보입니다. 하지만 아기가 보채거나 우유를 먹지 않거나 열이 나거나 하는 증상은 안보입니다. 무증상이지요.
- 기저귀도 천으로 바꾸었고 대변을 보고 난 후 위생상 깨끗하게 하려고 씻겨주고 해도 며칠 전 검사에서 대장균이 발견되었답니다.
- 왜 요로 감염이 치료가 안 되고 끊임없이 나타나는지 그에 따른 치료법이 무엇인지, 부모로서 평상시 요로 감염을 자주 앓는 아기를 어떻게 다루어야 하는지 등이 궁금합니다. 꼭 답변 부탁드립니다.
A.
백미께
- 안녕하세요. 질문해 주셔서 감사합니다. 좋은 질문입니다.
- 자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답변을 드리는 데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
- 연구에 의하면, 1차 검사한 소변 세균 배양 검사 결과에서 한 종류의 박테리아 집락이 십만 개나 그 이상이면, 요로 감염이 있을 가능성이 85%이고,
- 2차 실시한 소변 세균 배양 검사 결과에 바로 전 검사에서 발견된 박테리아와 같은 종류의 박테리아 집락이 십만 개나 그 이상 있으면, 요로 감염이 있을 가능성이 92%이고,
- 3차 실시한 소변 세균 배양 검사 결과 1, 2차 검사의 결과와 같은 종류의 박테리아 집락이 십만 개나 그 이상 있으면, 요로 감염이 있을 가능성이 98%입니다.
- 세균 배양 검사를 하기 위한 소변을 받을 때, 외음부를 비눗물로 잘 깨끗이 씻고, 가능하면 소변 볼 때 중간 소변 줄기 부분 소변을 받아서 소변 배양 검사를 해야 합니다.
- 그러나 신생아나 영유아의 소변을 배양 검사 할 때 사용할 이상적 피검물 소변을 받는다는 것은 상당히 힘듭니다(p.00 소변검사 참조).
- 1세 이전의 남아가 요로 감염에 한 번이라도 걸리면, 요로에 어떤 기형이 있을 가능성이 50% 또는 그 이상입니다.
- 두 번 이상 요로 감염에 걸렸으면, 요로의 어느 부위에 이상이 있을 가능성이 더 많습니다.
- 배뇨 방광 요도 조영술(VCUG), 요로 초음파, DMSA 스캔, IVP 등 여러 종류의 요로 검사 중 필요한 검사를 해야 합니다.
- 이런 각 검사에는 장점과 단점이 있고, 필요에 따라 선택적으로 이용합니다.
- 그 중 배변 방광 요도 조영술 검사가 필요할 때가 많습니다.
- 배변 방광 요도 조영술 검사 결과가 정상이고 요로 감염이 완치된 이후 요로 감염 증상이 없어도, 2주, 1개월, 3개월, 6개월 정도에 소변 화학 검사, 소변 세균 배양 검사를 하시기 바랍니다.
- 요로에 생긴 기형의 종류에 따라 수술 치료도 합니다. 때로는 장기간 항생제 복용을 해서 요로 감염 재발을 예방 합니다.
- 소변 세균 배양 검사 결과가 비정상으로 나왔다고 해서 그 검사 결과에 의존해서만 요로 감염에 거려 있다고 진단할 수 없습니다.
- 소변 화학 검사, 소변 세균 배양 검사와 증상 징후 등을 종합해서 요로 감염을 진단하고, 그에 따라 치료하는 것이 보통입니다.
- 천 기저귀를 쓰는 것을 더 권장합니다. 기저귀의 종류와 요로 감염은 별 관계가 없습니다. 외음부를 특별히 더 청결하게 할 필요는 없습니다. 손발 닦듯이 보통으로 청결하면 됩니다.
- 소아청소년과에서 진찰·진단을 받으시고, 이런 문제에 관해서 상담하시기 바랍니다.
- 요로 감염을 참조하십시오.
- 질문이 더 있으면, 다시 연락해 주시기 바랍니다.
- 감사합니다.
- 새해에 건강하시고 복 많이 받으시고 모든 일이 형통하길 빕니다. 이상원 드림
|
다음은“요로감염과 소변검사”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 요로감염과 소변검사
Q.
- 안녕하세여… 바쁘시겠지만, 자세한 답변 부탁드립니다.
- 4개월 된 아들이 고열로 2주 전 요로 감염으로 병원에 입원을 했다가 열흘째 퇴원을 했습니다. 입원 당시 만 하루만에 열은 떨어졌구여… 초음파와 역류검사에서는 이상이 없다고 하구여…
- 핵의학 검사에서 신장에 약간의 상처가 있다고 합니다. 주치의께서는 그 상처로 인해 아이의 생활에 지장이 있지는 않을 거라고 했지만, 걱정이 많이 됩니다.
- 병원에서 항생제(정맥주사??) 치료를 했는데, 워낙 어린아이다 보니 링거가 하루 이상을 가지 못해 열흘 째 퇴원해서 약물 치료를 하고 있습니다…
- 처음엔 2주 정도를 입원해야 한다고 했지만, 경과가 좋으면 열흘 후에 퇴원하여 약물치료도 가능하다고 했거든여… 퇴원해서 아이는 잘 놀구여, 열도 없구여, 설사는 약간 하거든여,,,,,
- 6월 7일 내원해서 소변검사 예약을 해 놓은 상태인데여… 자꾸만 신장의 상처가 마음에 걸리거든여,,, 괜찮을까여???
- 그리고 DPT소아마비 2차 예방 접종(5월 27일)을 해야 하는데, 아직 못하고 있거든여… 예방 접종은 어찌 해야 할까여???
A.
- 국 엄마께
- 안녕하세요. 좋은 질문해 주셔서 감사합니다.
- 자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답변을 드리는 데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
- 소아청소년의 요로 감염은 흔히 볼 수 있는 소아 감염병 중 하나입니다.
- 진단을 하기 위해서 신장·요관·방광의 초음파 검사를 하고, 신장이 정상보다 작은지 또는 신장 손상이 생겼는지 알아보기 위해서 신장 DMSA 스캔 검사를 하고, 방광 요관 역류가 있는지 알아보기 위해 배뇨 방광, 요도 조영술 검사를 하고, 소변 화학 검사, 소변 세균 배양 검사, 혈 중 BUN, 크레아티닌 농도 등을 필요에 따라 검사해서 요로 감염을 진단·치료할 수 있습니다.
- 이런 검사를 요로 감염과 그 증상 징후가 다 나은 후에도 필요에 따라 다시 추적 검사를 하기도 합니다.
- 요로 감염은 신장·요관·방광·요도 등에 선천성 기형이나 후천성 기형 또는 어떤 선행 병이 있을 때 재발될 가능성이 많이 있습니다.
- 신장 상흔이 생긴 정도는 그렇게 심하지 않은 것 같습니다. 담임 소아청소년과 의사와 상의해서 차후에 검사를 또 해볼 수 있습니다.
- 앞으로 열이 나거나 구토, 설사, 성장지연 등으로 어떤 치료를 받아야 할 때는 치료 받기 전에 가능한 한 소변검사를 우선적으로 해서 요로 감염이 재발됐는지 확인하는 것이 아주 중요합니다.
- 이 나이에는 DTaP, B형 간염, 소아마비, 로타바이러스 감염, 히브, 폐렴 예방접종을 적어도 2차 받아야 합니다.
- 소아청소년과에서 진단·치료를 받으시고, 이런 문제에 관해서 상담하시기 바랍니다. [부모도 반의사가 되어야 한다–소아가정간호백과]-제2권 소아청소년 질병과 안전사고의 예방, 제3권 신생아, 영유아, 학령기와 사춘기 아이들의 성장발육–해당 연령의 성장 발육, 생후 1개월~6세 아이들의 발육 이정표. 제4권 모유, 모유수유, 이유. 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방.
- 요로 감염 등을 참조하시기 바랍니다.
- 질문이 더 있으면, 다시 연락해 주시기 바랍니다. 감사합니다. 이상원 드림
|
다음은“요로 감염,소변 세균 배양검사”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 요로 감염,소변 세균 배양검사
Q.
- 안녕하세요.. 또 이렇게 편지를 보내는군요. 이번에도 균이 나왔다고 하더군요. 우리 아이는 이제 막 2달이 조금 넘었습니다. 우리 아이는 열두 없고, 우유도 잘먹습니다. 그런데 자꾸 소변검사만 하면 균이 나온다구 합니다. 균의 종류에서 3등급 정두 되는 균이라구 합니다. 그래서 이번에두 소변검사에서 또 균이 나오면 약을 먹구 다른 검사를 한다구 합니다. 자꾸 걱정이 됩니다. 이런 경우, 우리 아이는 어떤 증상인가요. 정말 걱정 많이 됩니다. 잘 먹구 하는데, 자꾸 균이 나와서 말입니다. 선생님은 아무래두 소변이 깨끗이 나오지 않구 고여 있다가 나오는 것 같다구 합니다. 아무래두 검사는 해 봐야 하겠지만 말입니다. 선생님, 어떻게 해야 하나요.
- A.
- 행미님
- 안녕하세요. 질문해 주셔서 감사합니다. 좋은 질문입니다. 자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답변을 드리는 데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
- 요로 감염을 진단하기 위해 소아청소년들의 소변을 받는 데 상당한 시간과 기술이 필요합니다.
- 대변이 외음부에 눈곱만큼이라도 묻어 있을 때 영아 소변 주머니(사진 1-34, 1-35)로 받은 소변, 외생식기를 적절히 씻지 않고 받은 소변, 받은 후 한두 시간 이상 실내 온도에 방치했던 소변 피 검물, 불결한 용기에 받은 소변 피 검물 또는 불결한 손으로 만진 소변 피 검물로 소변 세균검사를 하면, 검사 결과가 비정상으로 나올 수 있습니다.
- 이런 이유로, 필요에 따라 요도를 통해 뇨 카테터를 방광 속에 넣어 방광 속에 든 소변을 채취해서 그 소변으로 세균 배양 검사를 할 때도 있고, 때로는 복벽을 통해 주사바늘로 방광 속 소변을 직접 뽑아 소변 세균 배양 검사를 합니다.
- 요로 감염이 있을 때 소변 세균 배양 검사 결과가 비정상으로 나타날 때도 있고, 세균 배양 검사에 사용한 소변 피 검물로 소변 화학 검사를 하면 백혈구가 비정상적으로 많이 나오고 적혈구도 많이 나올 수 있고, 세균이 비정상적으로 많이 있는 것이 보통입니다.
- 다시 말씀드리면, 요로 감염이 있을 때 소변 화학 검사 결과의 대부분이 비정상으로 나옵니다.
- 소변을 어떻게 받아서 소변 세균 검사를 했는지, 소변 화학 검사 결과는 어떻게 나왔는지, 소변을 현미경으로 검사했을 때 검사 결과는 어떻게 나왔지 알고 싶습니다.
- 항생제 치료를 시작하기 전, 첫 번째 즉 1차 세균 배양 검사의 결과가 비정상적으로 나왔을 때 요로 감염에 걸려 있을 확률은 60% 정도뿐이고,
- 2차 세균 배양 검사 결과가 비정상적으로 나왔을 때 요로 감염에 걸렸을 확률은 90% 정도이며,
- 3차 세균 배양 검사를 했을 때 1, 2, 3차 결과가 모두가 비정상으로 나올 때 요로 감염에 걸렸을 확률은 98% 정도입니다.
- 이런 이유로, 영유아의 경우, 단 한 번 소변 세균 배양 검사 결과로 요로 감염 유무를 확진하기가 어렵습니다.
- 주사바늘로 빼낸(치골 상부 소변 흡입) 소변 피 거물로 소변 세균 배양 검사와 소변 화학 검사 하여 그 검사 결과가 비정상이면, 신장 요관 방관 초음파 검사, 배뇨 방관 요도 조영술, DMSA 신장 스캔 등으로 신장·요관·방광·요도 등에 선천성 기형이 있는지, 요로 감염 등으로 신장이나, 요관의 어느 부위가 어느 정도로 손상되어 있는지 알아보겠습니다.
- 이런 검사를 언제든지 다 할 필요는 없습니다. 그러나 신장 요관 방관 초음파 사진, 배뇨 방관 요도 조영술, DMSA 신장 스캔 검사를 다시 하든지, 만약 안 했으면 꼭 해보는 것이 좋을 것입니다.
- 비록 첫 번째 소변 세균 배양 검사의 결과가 정상이어도, 적어도 한 번 더 추적 검사를 해보는 것이 좋을 것 같습니다.
- 소변 세균 배양 검사 결과에 따라 적절한 항생제로 적어도 6개월 내지 1년 동안 요로 감염을 치료·예방하는 것도 생각해 볼 수 있습니다.
- 아시겠지만, 이런 경우에 비뇨기과 전문의와 상의해서 치료할 때도 있지만, 소아 신장과 전문의와 상의해서 치료하는 것이 좋다고 생각됩니다.
- 이런 치료에도 그때그때의 상황에 따라 진단·치료 방법이 다르다는 것을 말씀드리고 싶습니다.
- 요로 감염을 참조하시기 바랍니다.
- 질문이 더 있으면, 다시 연락 주시기 바랍니다. 감사합니다. 이상원 드림
|
다음은“요로 감염, 소변 세균 배양검사, 상담 후 상담”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 요로 감염, 소변 세균 배양검사, 상담 후 상담
Q.
- 오늘 아침 동네 소아청소년과 에서 소견서를 받아 종합병원에 갈 생각으로 갔더니 선생님께서 큰 병원에 갈 정도는 아니라고 하십니다. 우리 아이는 요로 감염이 아니라고 하십니다.
- 선생님 말씀이 소변에 혈구가 섞여 나오는데, 아직은 관찰할 단계라고 하십니다.
- 유전적으로 가족 중에 그런 사람이 있어 그럴 수도 있다고 하시면서 6개월 정도는 지켜봐야 된다고 하십니다.
- 엄마 입장에서는 영 시원하지가 않군요.
- 이비인후과를 전문으로 하시는 선생님이 보셨는데, 목이 상당히 많이 부어 있어 고열이 날 수 있다고 하십니다.
- 목약과 해열제를 받고 왔습니다.
- 선생님의 홈페이지 중에 우리 아이가 아파요 중에서 1.비뇨생식기 질환(혈뇨)을 읽었습니다. 우리 아이인 경우 잠재 혈뇨 같은데 계속 관찰만 해도 되는 건지 다시 한 번 답변을 부탁드립니다.
- 잠재 혈뇨 중에서도 여러 가지 이유가 있지 않을까요? 빨리 세밀하게 검사를 해야 되는 것은 아닌지?
- 소아청소년과 에서 하는 소변검사만으로도 그것이 무해성 혈뇨인지 알 수 있나요?
- A.
미화님께
- 질문을 또 해 주셔서 감사합니다.
- 지금쯤 많이 혼동하실 줄 압니다. 저도 많이 혼동하고 있습니다.
- 제가 인터넷으로 건강 상담하면 이런 혼동이 생길 것이라고 생각해서 두려워했습니다.
- “소변에 피가 섞여 나오고, 배가 아프고, 소변을 자주 보기에, 병원에 가니 방광염이라면서” 정보를 저한테 주셨습니다.
- 소아청소년과에서는 “방광염이 있다.”라고 진단하는 대신 “요로 감염”이란 병명을 더 많이 쓴다고 말씀드렸습니다.
- 즉, 자녀분께 요로 감염이 있었다고 말씀을 들었습니다. “소아에게 요로 감염에 걸렸던 과거 병력이 있으면 요로 감염에 또 걸릴 가능성이 더 있습니다.”라고 말씀드렸던 것 같습니다.
- 소변검사(Urinalysis), 소변 세균 배양 검사(Urine culture for bacteria) 결과가 비정상으로 나왔다고 해서 100%로 요로 감염에 걸렸다고 100% 진단할 수 없습니다.
- 그러나 증상 징후가 있으면서 소변검사와 소변 세균 배양 검사 결과가 비정상이면(같은 종류의 세균 집락이 십만 개나 그 이상), 요로 감염에 걸렸을 가능성이 있다고 봅니다.
- 다시 말씀드리면, 자녀가 당시에 요로 감염에 걸려 있었다고 확진을 할 수는 없다는 뜻입니다.
- 왜냐하면 33개월 된 여 유아의 외생식기에 염증이 있을 때도, 소변을 볼 때 아플 수 있고 소변이 자주 마렵고 소변에 농뇨와 혈뇨가 나올 수 있습니다.
- 또 소변 세균 배양 검사를 할 피 검물용 소변을 받을 때 소변 속으로 극소량의 대변이 묻어 들어갈 수 있습니다. 그런 소변으로 소변 세균 배양 검사를 했을 때, 세균 배양 검사에 자란 세균이 신장이나 방광에서 나온 세균으로 잘못 판정할 수 있습니다.
- 이런 이유로, 어린 영유아들의 요로 감염을 진단할 때에는 항생제 치료를 시작하기 전에 소변을 단 한번 받아 소변 세균 배양 검사를 해서 요로 감염을 진단하는 것 보다, 때로는 두서너 번 소변을 받아 소변검사를 두세 번 하고 소변 세균 배양 검사도 두세 번 할 수 있습니다.
- 어떤 때는 소변 검사 결과가 정상적이지만 요로 감염이 있을 수 있고, 소변 세균 배양 검사 결과가 비정상인데도 요로 감염이 없을 수 있습니다.
- 말씀을 더 드리면 더 복잡해 질 수 있습니다.
- 소변에 잠재성 피가 섞여 나오는 원인은 많이 있습니다.
- 우유를 먹을 때 생긴 요로 알레르기, 바이러스 요로 감염, 결핵성 요로 감염, 콩팥 타박상, 사구체 신염, 육체적 운동, 박테리아 요로 감염, 알레르기성 질환, 고 칼슘증, 종양, 기생충증, 요로 이물질, 출혈성 질환 등의 많은 원인에 의해서 혈뇨가 생길 수 있습니다.
- 몸에 아무 이상이 없는데도 혈뇨만 있을 수 있습니다. 이런 혈뇨를 양성 잠재 혈뇨라고 합니다.
- 혈뇨가 날이 갈수록 더 심해지거나 잠재 혈뇨를 멀티스틱스 화학 검사로 측정했을 때 검사 결과가 1+~ 4+까지 있습니다. 그 중 몇 (+)인지에 따라 원인과 진단·치료 방법이 다릅니다.
- 혈뇨만 나오는지 혈뇨와 단백뇨가 동시 나오는지, 또는 혈뇨와 농뇨가 동시 나오는지에 따라 진단·원인 치료가 다릅니다.
- 요약하면, 혈뇨의 원인이 많고, 혈뇨의 원인을 정확하게 찾아내기가 때로는 쉽지 않습니다.
- 편도가 부어서 열이 났다고 하니 지금은 다 회복되었으리라 믿습니다.
- 편도염이 A군 베타 용혈성 연쇄상구균으로 생겼으면, 사구체 신염도 의심해 보아야 합니다. 또 열로 인해 생기는 열성 혈뇨도 있습니다.
- 비뇨기계에 어떤 종류의 기형도 없이 방광염 등 요로 감염을 앓을 수도 있습니다.
- 현재 혈뇨가 있기 때문에, 혹시나 혈뇨와 먼저 번 앓았던 요로 감염과 어떤 관련이 있는지 의심해 볼 수 있습니다.
- 또 비뇨기계에 어떤 이상이 없다고 100% 배제할 수 없습니다.
- 어떤 의사는 요로 감염을 한번만 앓아도 비뇨기계에 어떤 이상이나 선행 질병이 있어서 요로 감염이 생겼는지 알아보는 것이 좋다고 주장합니다.
- 참 복잡하지요.
- 만약에 자녀가 제 딸이라면 신장·요관·방광 초음파 검사를 2~3주 내에 해보겠습니다. 그리고 소변을 잘 채취해서 소변검사와 소변 세균 배양 검사를 하고, 검사 결과가 정상이면서 소변에 피가 (+) 정도 또 나오면 걱정하지 않고 관찰 치료를 하겠습니다.
- 그러나 소변에 피가 (+) 이상 더 나오고 다른 검사 결과가 비정상이면, 적극적으로 비뇨계통에 어떤 이상이 있나 검사를 하겠습니다.
- 소아청소년과에서 다시 진찰·진단·치료를 받고 상담하시기 바랍니다.
- 혼동하게 해드려서 죄송합니다.
- 질문이 더 있으면, 또 방문하세요.
- 감사합니다. 이상원 드림
Urinary tract infections (UTI) 요로 감염
Urinary Tract Infections and Terms
• Urinary tract – The kidney, ureter, bladder, and urethra are called the urinary system, urinary system, urinary tract, or urinary tract.
• Nephritis – An infectious disease in which pathogen infections, such as bacterial or viral infections, occur only in the kidneys is called nephritis.
• Pyelonephritis – When a pathogen infection such as a bacterial or viral infection is simultaneously infected with the kidney and kidney, it is called pyelonephritis.
• Cystitis – An infectious disease in which pathogen infections such as bacterial or viral infections occur only in the bladder are called cystitis.
• Urethritis – An infectious disease that occurs only in the urethra with pathogen infections such as bacterial or viral infections is called urethritis.
• Urinary tract infections—Infectious diseases of the entire urinary tract (kidney, ureter, bladder, urethra) are sometimes diagnosed as urinary tract infections, and infectious diseases that occur only in part of the urinary tract are diagnosed as urinary tract infections.
• Asymptomatic urinary tract infections – If you have a urinary tract infection but no symptoms, it is called asymptomatic urinary tract infections. In fact, it is not asymptomatic, but there are symptomatic signs, but it can be said that it is a urinary tract infection that is not aware of the presence of a urinary tract infection. Dissection of the urinary system and urinary tract infection in children and adolescents
(Figure 1-36)
Figure 1-36. The kidneys, ureters, bladder and urethra are called the urinary tract. An infection that occurs in part or all of the urinary tract is called a urinary tract infection. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
• Especially in the case of infants and toddlers, the distance from the kidney to the bladder and the distance from the kidney to the outer urethra of the urethra is much shorter than that of adults, and infants and toddlers have weak immune system function to defend against infectious diseases that can resist infection by pathogens such as bacteria and viruses. , For a number of other reasons, infants, especially infants, are more susceptible to urinary tract infections.
• In addition, urinary tract infections are more likely in infants and young children due to congenital malformations or acquired abnormalities in the urinary system.
• When a bacterial infection occurs in the urinary tract of an infant, the bacteria are confined to a portion of the kidney, bladder, ureter, and urethra, so that infection does not occur. It is common to develop urinary tract infections in which the entire urinary tract is simultaneously infected.
• Just as the entire nasal cavity, sinuses, pharyngeal cavity, adenoids, and tonsils, which are not infected with the virus only in the nasal cavity, are infected when a cold occurs. When the urinary tract of young infants is infected with bacteria, bacterial nephritis, bacterial pyelitis, bacterial cystitis, bacterial urethritis It is rare that this occurs separately.
Incidence of urinary tract infections
• Newborns 1-4 days old: 1%
• Infants: 2%
• School-age girls: 1.1%
• Young women: 1%
• Pregnant women: 5%
• Men over 60: 1.6%, Source: David Scheifele, M.D
Causes of urinary tract infection
• Acute urinary tract infection in children and adolescents (ages 0-18) is one of the most common acute infectious diseases in children and adolescents.
• 3.3% of boys and 6.5% of girls before the age of 1 have acute urinary tract infections.21 (Reference; differences from the above information).
• Bladder ureteral reflux is found in 30 to 40% of urinary tract infections in children and adolescents.
• If urinary tract infections in children and adolescents caused by bladder ureter reflux are not properly treated, urinary tract infections may recur and sequelae such as high blood pressure, kidney damage and kidney scarring may occur .
Pathogens and routes of infection that can cause urinary tract infections in children and adolescents
• E. coli is 80%,
• The rest are Klebsiella,
• Enterobacter
• Streptococci,
• Proteus,
• pseudomonas,
• Enterococci, Serratia, Heralia, Staphyloccocus Aureus, and other bacteria can more commonly cause urinary tract infections.
• After infection of one type of bacteria among several types of bacteria or more than one type of bacteria at the entrance of the urethra → the bacteria infect the entire urinary tract in the order of urethra → bladder → ureter → kidney, etc., causing urinary tract infection. This is the most common route of infection.
• Rarely, a urinary tract infection can also be caused by a Candida fungal infection.
• Pathogens such as bacteria that caused infectious diseases of organs or tissues other than the urinary system, or pathogens such as bacteria that caused sepsis along the bloodstream can cause secondary infection of the kidneys, resulting in pyelonephritis.
• The bacteria that cause pyelonephritis can continue to spread in the kidneys, in the order of the kidneys → ureters → bladder → urethra, and infect the entire urinary tract.
• The distance between the external urethra and the anus in girls is much shorter anatomically than in boys, and due to normal hygiene management problems, and the unusual anatomy of the vulva and urinary tract, girls are infected with the external urethra by E. coli in the stool. You can get urinary tract infections more easily and more often than boys.
• Having a habit of wiping the anus from the anus to the vulva after having a bowel movement, especially women and infants, are more susceptible to urinary tract infections.
• The incidence of urinary tract infections in male and female newborns and those in male and female infants before 1 year of age are almost the same, but the incidence of urinary tract infections in female infants after the first birthday is much higher than that of male infants. high.
• If you have congenital urinary malformations such as kidney, ureter, bladder, or urethra, such as double ureter, ureteral flow, diverticulum, posterior urethral valve, bladder ureteral obstruction, or congenital neurogenic bladder or acquired neurological bladder or muscle abnormalities, You are more susceptible to infection.
Table 1-3. Symptoms of urinary tract infection with age (%) 표 1-3. 나이에 따른 요로 감염의 증상 징후(%)
| Symptoms, signs of urinary tract infection | From birth to 1 month After birth | 1 month to 2 years | 2 to 5 years | 5 to 12 years |
| Growth impairment, growth retardation, | 53% | 36% | 7% | – |
| Irritability, colic | – | 13% | 5% | – |
| Urine smells, urine is cloudy | – | 8% | 14% | – |
| Diarrhea | 18% | 16% | – | – |
| Vomiting | 25% | 29% | 16% | 3% |
| Fever | 11% | 38% | 57% | 50% |
| Convulsions | 2% | 6% | 9% | 5% |
| Hematuria | – | 6% | 16% | 6% |
| Frequent urination, difficulty urinating | – | 4% | 34% | 40% |
| enuresis | – | – | 27% | 29% |
| Abdominal pain | – | – | 23% | 44% |
| Frank pain | – | – | – | 12% |
Source: Riley H.D. Pyelonephritis in children, Hospital practice 3, 1972.
Symptoms, signs of a urinary tract infection
• The severity of the urinary tract infection, predecessor disease before the occurrence of urinary tract infection, acute urinary tract infection or chronic urinary tract infection, the age of the child (age, age, age, etc.), the type of bacteria that caused the urinary tract infection, the presence or absence of congenital urinary tract deformities, and Symptoms and signs of urinary tract infection vary greatly depending on the severity and the like.
• When newborns, infants, and infants have acute urinary tract infections or chronic urinary tract infections, such as fever, difficulty urinating, urinating frequently, hematuria, pale urine, foul-smelling urine, peeing day or night, pain in the belly or side Symptoms may appear.
• A variety of other symptoms can result from a urinary tract infection, such as:
• Difficulty eating well for no apparent reason, fluffiness, mild or high fever suddenly occurs, such a fever may come on for several days and then no longer develop, a fever may occur for some time a day and then no longer, and weight is not gaining normally, They may not be much bigger than their peers.
• Sometimes, symptoms that are not related to the usual symptoms of urinary system disorders such as high fever, vomiting, abdominal pain, diarrhea, and competition may appear suddenly. • Often it is not clear if you have a urinary tract infection without having to test the urine of a child with a urinary tract infection.
• In some cases, especially infants and toddlers are misdiagnosed as having gastroenteritis, cold, otitis media, or flu, and are treated with antibiotics without knowing whether they have a urinary tract infection.
• Some of the 2 to 3-year-old girls with urinary tract infections can’t cover their urine when they can cover their urine, and they can pee on clothes day and night.
• Among some infants and toddlers with urinary tract infections, the vulva may be red and red, and the urine may have a bad smell.
• If a school-age child has a urinary tract infection, they may urinate frequently, urinate, and complain of pain in the belly. • When urinating, there are cases where it hurts to urinate well, and the belly may be bloated. • You may have a high fever for several days and hurt one side or both sides.
• The urine may contain red blood, and there are times when very small amounts of blood come out.
• A urine microscopic bacteriological test will tell you if there are bacteria in your urine, and Multistick urine chemistry will tell you the blood is in your urine.
• When you have a urinary tract infection like this, sometimes the naked eye cannot see if there is blood in the urine, and the blood in the urine can be seen under a microscopic examination. Also, if you have a urinary tract infection, a small amount of blood can be seen in the urine, and sometimes red blood can be seen in the urine.
• The urine contains a lot of white blood cells, which can cause the urine to turn pale.
• Acute urinary tract infections can lead to chronic urinary tract infections if not treated promptly and appropriately.
• If urinary tract infections are not treated early and appropriately, acute urinary tract infections can become chronic pyelonephritis, abnormally high blood pressure can lead to secondary hypertension and anemia.
• If chronic pyelonephritis is not properly treated, some or all of the kidneys may be temporarily or permanently damaged, and urinary tract infections may be cured only by surgically removing the entire damaged kidney.
Diagnosis of urinary tract infection
Photo 1-37. Urine for the specimen is received in a sterile cup and subjected to a urine chemistry test, a urine microscopic bacterial test, a urine bacterial culture test, and an antibiotic susceptibility test. Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Photo 1-38. Urine bacterial culture can be tested with urine. A bacterial antibiotic susceptibility test is performed on the grown bacteria. The ideal treatment is to treat urinary tract infections with antibiotics that are most effective according to the results obtained from bacterial antibiotic supervision tests. Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
• If you suspect that you have a urinary tract infection based on your medical history, symptoms, symptoms, and examination findings, it is common to diagnose it with a multistick urine chemistry test, a microscopic urine test, and a urine bacterial culture test.
• Urine for bacterial culture testing should be obtained in clean, sterile cups. • Ideally, if possible, do a urine bacterial culture test to find out what kind of bacteria are causing the urinary tract infection, and to do a bacterial antibiotic susceptibility test to select and treat the most appropriate antibiotic based on the test results. • Whether the urinary tract infection is acute or chronic, the diagnosis method differs depending on the age of the child with urinary tract infection and the preceding abnormalities or diseases that caused the urinary tract infection.
• If an infant or toddler before 2 years of age has an acute urinary tract infection, • kidney ultrasound and • Voiding cystourethrography (VCUG) test
• Or, it is recommended to diagnose a urinary tract infection by performing a radionuclide bystander urethrography as a basis, and to find out if there is any abnormality in the urinary tract.
• An ultrasound of the kidneys can determine if you have hydrocephalus or other types of anatomical abnormalities or malformations of the kidneys, but an ultrasound of the kidneys is inappropriate for determining if you have bladder ureteral reflux.
• A DMSA kidney scan can help determine which areas of the kidney are damaged and to what extent.
• Intravenous pyelography (IVP) is a rare test these days.
• Very rarely, if necessary, a urologist puts a cystoscope with a special mirror into the bladder through the urethra and visually sees the urethra and the inside of the bladder through the cystoscope. It is also diagnosed and treated to see if there is any.
• Sometimes urine chemistry and microscopic urine test cannot confirm a urinary tract infection. Therefore, urine chemistry and microscopic urine tests are repeated two or three times to confirm urinary tract infections.
Table 1-4. Bacteriuria% according to age Age (age or age) Incidence rate (%) 표 1-4. 나이에 따른 세균뇨(Bacteriuria) %
| age | incidence rate(%) | Male and female incidence rate |
| From birth to 1 month (newborns) | 1% | 1.5(Male) : 1(female) |
| 1 month to 2 years old (infants and toddlers) | 2% | 1.5(female) : 1(Male) |
| 2-5 years old (infants and preschool children) | 1~2% | 4.8(female) : 1(Male) |
| 5 to 16 years old (school-age children and adolescent children) | 1~2%(female) 0.05%(Male) | 1.5(Male) : 1(female) |
Sources and references D. Heller’s lecture at Havard Medical School
See Bacteriuria
First urinary tract infection and urinary bladder urethrography (VCUG) examination in children and adolescents
• Urinary tract infections can occur when there are no prior abnormalities or diseases in the urinary tract. • However, urinary tract infections are more likely to occur if there are some congenital or acquired abnormalities in the urinary tract.
• Ultrasonography can be used to check the size of the kidneys and whether or not bladder ureteral reflux is present. However, sometimes accurate test results may not be available.
• When the first urinary tract infection occurs in children and adolescents, it is a matter of controversy in the medical community whether urination bladder urethrography should be performed or not. However, it is usually recommended to do the test these days.
• A urinary bladder urethra examination can help determine if there is a bladder ureteral reflux. • Kidney ultrasound results are more reliable than urination cystourethrography results in determining if the kidney is swollen, if there is a wound, scar, or hydronephrosis, if the kidney is normal in size, and if there is bladder ureteral reflux.
• Therefore, when the first urinary tract infection occurs in children and adolescents, it is advisable to perform urinary bladder urethrography and renal ureteral bladder ultrasonography.
• It is up to your doctor’s discretion as to what type of test to take and to what extent (see Bladder Uterine Reflux).
Photo 1-39. Picture of an intravenous pyelogram examination. a-left and right kidneys, b, c-left and right ureters. Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Photo 1-40. Intravenous pyelography examination picture. a-left and right ureters, b-dual ureters, middle and upper double ureters, c-dual ureters, middle and lower double ureters, d-right kidneys, e-left kidneys. Copyrightⓒ 2011 John Sangwon Lee, MD.FAAP
Photo 1-42. Urinary bladder urethrography test picture-There is an abnormally large amount of urine in the left kidney and the kidney is damaged. a-damaged kidney, b-normal bladder. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 1-41. Urination bystander urethral angiography picture. The left ureter is abnormally dilated. a-right ureter, b-left ureter, c-bladder. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Treatment and prevention of urinary tract infections
• Treatment differs depending on the symptoms and severity of urinary tract infections, the presence of congenital urinary tract malformations, causes, and complications.
• If an infant or school-age child has a high fever and is severely ill due to an acute urinary tract infection, it is common to be admitted to a hospital and treated with an appropriate antibiotic vascular injection
. • Studies have shown that the results of adequate treatment of acute urinary tract infections in children and adolescents with oral antibiotics and the results of treatment with appropriate vascular antibiotics are almost the same. So, in recent years, there is a tendency to treat acute urinary tract infections with oral antibiotics .
• Urinary tract infections with no fever and no symptoms may be treated for 10 days with amoxacillin or baktrim or other appropriate antibiotics as prescribed by a doctor. Kidney, urethra, bladder ultrasonography, urination cystourethrography, or intravenous pyelography for children who have a urinary tract infection for the first time, or with a past history of having a urinary tract infection at least once in the past. It is good to check whether the ureter, bladder, and urethra are normal.
• This is because a significant number of children and adolescents who have had more than one urinary tract infection may find that they have congenital urinary tract anomalies or some acquired abnormalities in the urinary tract.
• Most boys with urinary tract infections after their first birthday are more likely to have congenital malformations of the urinary tract. Therefore, if a boy has a urinary tract infection after the first childbirth, the entire urinary system is examined using an ultrasound examination of the urinary tract such as kidney, ureter, bladder, intravenous pyelography, kidney X-ray, CT scan, etc. Is recommended.
• Children who have had one urinary tract infection in the past may have a urinary tract infection frequently. That’s why it’s a good idea to regularly follow up with urine chemistry tests, microscopic urine tests, and urine bacterial culture tests.
• When urinary tract infections recur frequently, the original pre-infectious disease causing the cause is treated with appropriate antibiotics, and then prophylactic treatment is continued for months to several years with nitrofurantoin or sulfa drugs. It was recommended to prevent recurrence of urinary tract infections.
• However, recent studies have shown that even if urinary ureteral reflux is present and urinary tract infection recurs, prophylactic treatment with prophylactic antibiotics is not necessary.
• For children with severe bladder ureteral reflux and a history of recurrent urinary tract infections, it is recommended that prophylactic antibiotic therapy may be selectively administered.
• Cefixime urinary tract infection prophylactic treatment is more effective than nitrofurantoin urinary tract infection prophylactic treatment. Conversely, the side effects of nitrofurantoin urinary tract infection prophylactic treatment are when Cefixime urinary tract infection prophylactic treatment It occurs less than the side effects of 22.
• Studies have shown that prophylactic treatment for urinary tract infections with a small amount of Trimethoim-sulfamethoxazole for a long period of time reduced the incidence of recurrent urinary tract infections (Source: NEJM October 29, 20097 p.17490).
• As explained above, there are several methods of prophylactic treatment for urinary tract infections. To the last, the doctor in charge should choose the appropriate treatment method at the right time. • In the case of mild bladder ureteral reflux, it is recommended to have a VCUG test every 2 years while prophylactic treatment for urinary tract infections with antibiotics, and every 3 years for moderate to severe bladder ureteral reflux.
• See Nitrofurantoin
• NICE USA The latest diagnostic treatment guidelines for the diagnosis, treatment, and prevention of urinary tract infections in children and adolescents (under 16 years of age) have been published, but there is debate about the guidelines (2007)23.
The following is the guideline for diagnosing and treating urinary tract infections in children and adolescents in the United States.
• If a urinary tract infection develops in an infant under 3 months of age, it is recommended to consult a pediatric and adolescent infection department to receive vascular antibiotic treatment. However, it is recommended to treat pyelonephritis in infants older than 3 months with oral antibiotics for 7 to 10 days.
• Infants older than 3 months of age who develop cystitis or lower urinary tract infection are recommended to be treated with oral antibiotics for 3 days.
• Conventional antibiotic prophylactic treatment is no longer recommended.
• Conventional imaging tests to diagnose bladder ureteral reflux are no longer recommended.
• If you begin to treat urinary tract infections in infants over 6 months of age, and if the treatment is effective, it is recommended that you do not need to perform a routine ultrasound examination.
• However, if the treatment of a urinary tract infection in infants under 6 months of age is not treated and the treatment is not effective, it is recommended to perform an ultrasound examination within 6 weeks.
• If you have recurrent urinary tract infections, complications of urinary tract infections, or atypical urinary tract infections, it is recommended that you do an ultrasound while you are acutely ill.
• When infants and toddlers under 3 years of age have recurrent urinary tract infections, complications of urinary tract infections, or atypical urinary tract infections, it is recommended to perform a DMSA test 4-6 months after diagnosis.
• In this way, information on recommendations regarding the diagnosis, treatment, and prevention of urinary tract infections can also be confusing.
• I think it’s best to treat a urinary tract infection according to your doctor’s instructions.
The course of urinary tract infection
• Urinary tract infections that occur without blocking any part of the entire urinary tract can be cured in most cases.
• When there is a congenital malformation in the urinary tract and a urinary tract infection, 60% can be cured through medical and surgical treatment.
• Recurrent urinary tract infections or chronic urinary tract infections are cured by nearly 50% with long-term follow-up treatment.
• 22% of persistent urinary tract infections occur.
• 8% develop kidney failure. (From D. Heller’s Lecture on Pediatrics and Training Education)
Recurrence of urinary tract infection
• o 80% of urinary tract infections recur. o If properly treated each time, urinary tract infections can be relieved in 20-25% and may recur after 2 years.
o In adult women, 65% may recur after intercourse. (From D. Heller’s Lecture on Pediatrics and Training Education)
The following is an example of a question-and-answer for pediatric and adolescent health counseling on the Internet about “Urinary Tract Infections and Urine Tests”.
Q&A.
Urinary Tract Infection and Urine Test
Q.
• Good morning? After seeing your kind answer, I also post like this. Please sincerely answer.
• It’s a baby boy who has been born for 100 days. He was born and was admitted to the hospital for jaundice, and then for another week because of a urinary tract infection. He was diagnosed with kidney malformations, so he performed isotopes, kidney and bladder x-rays, and bacterial cultures.
• However, after a week of medication, I have a urinary tract infection again a few days later with fungi and then E. coli. However, I don’t see any symptoms such as the baby’s fuss, not eating milk, or having a fever. It is asymptomatic.
• I changed my diaper to a cloth, and even if I washed my stool for hygiene cleansing, E. coli was found in the test a few days ago.
• I wonder why urinary tract infections are not curable and constantly appear, what treatments are appropriate for them, and how to deal with babies with frequent urinary tract infections as a parent. Please answer me. A. White rice
• Good morning. Thanks for asking. That’s a good question.
• The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
• Studies have shown that if there are 100,000 or more colonies of one type of bacteria in the results of a urine bacterial culture on the first test, you are 85% likely to have a urinary tract infection,
• If the result of the second urine bacterial culture test shows 100,000 or more colonies of bacteria of the same type as the bacteria found in the previous test, then there is a 92% chance of a urinary tract infection.
• If there are 100,000 or more colonies of bacteria of the same type as the results of the first and second tests as a result of the third urine bacterial culture test, then you have a 98% chance of having a urinary tract infection.
• When receiving urine for a bacterial culture test, the vulva should be thoroughly washed with soapy water and, if possible, a urine culture test by receiving urine from the middle part of the urine stem when urinating. • However, it is quite difficult to receive urine from an ideal specimen for use in culture testing of urine from newborns or infants (see p.00 Urinalysis).
• If a boy before the age of 1 has a urinary tract infection at least once, he or she is 50% or more likely to have some abnormality in the urinary tract.
• If you have a urinary tract infection more than once, you are more likely to have an abnormality in any part of the urinary tract.
• Among the many types of urinary tract tests, such as urination cystourethrography (VCUG), urinary tract ultrasound, DMSA scan, and IVP, you will need to do the tests you need.
• Each of these tests has its strengths and weaknesses, and it is selectively used as needed.
• In many cases, a defecation bladder urethrography is required.
• Even if the results of the defecation bladder urethrography test are normal and there are no symptoms of urinary tract infection after the urinary tract infection is cured, we recommend that you do a urine chemistry test and a urine bacterial culture test at about 2 weeks, 1 month, 3 months, and 6 months.
• Depending on the type of malformation in the urinary tract, surgical treatment is also performed. Sometimes long-term antibiotics are taken to prevent recurrence of urinary tract infections.
• Just because a urine bacterial culture test result is abnormal, you cannot diagnose that you have a urinary tract infection only by relying on the test results.
• It is common to diagnose a urinary tract infection by combining urine chemistry tests, urine bacterial culture tests, and signs of symptoms, and treated accordingly. • It is more recommended to wear cloth diapers. There is little relationship between diaper type and urinary tract infection. There is no need to clean the vulva in particular. Just like cleaning your hands and feet, you just need to be clean.
• Get medical examination and diagnosis at the Department of Pediatrics and Adolescents, and consult with you about these issues.
• See Urinary Tract Infection.
• If you have more questions, please contact us again.
• Thank you. • May you be healthy and blessed in the new year and all things prosper. Lee Sang-won .MD
The following is an example of a question-and-answer for pediatric and adolescent health counseling on the Internet about “Urinary Tract Infections and Urine Tests”.
Q&A.
Urinary Tract Infection and Urine Test
Q.
• Hello… You may be busy, but please give me a detailed answer.
• My four-month-old son was admitted to the hospital for a urinary tract infection two weeks ago due to a high fever, and was discharged on the tenth day. At the time of hospitalization, the fever fell in just one day… There is no abnormality in the ultrasound and reflux test…
• Nuclear medicine tests say there are minor scars in the kidneys. My doctor said that the wound would not interfere with my child’s life, but I am worried a lot.
• I was treated with antibiotics (intravenous??) at the hospital, but since I am a very young child, Ringer has been discharged for 10 days and is taking medication because he has not been away for more than a day…
• At first, I said that I had to be hospitalized for about 2 weeks, but if the progress is good, I was discharged after 10 days and said that drug treatment was also possible… Since discharged, the child plays well, has no fever, has a little diarrhea,,,,,
• I came to the hospital on June 7th and made an appointment for a urine test… I keep getting hurt in my kidneys. Would it be okay???
• And I have to do the DPT polio 2nd vaccination (May 27th), but I haven’t been able to… What should I do with vaccination???
A.
• Dear Mom
• Good morning. Thanks for the great question.
• The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
• Urinary tract infection in children and adolescents is one of the most common childhood infectious diseases.
• Ultrasound examination of the kidney, ureter, bladder to diagnose, kidney DMSA scan to see if the kidney is smaller than normal or if there is kidney damage, and urinary bladder and urethra angiography to see if there is bladder ureter reflux. Urinary tract infections can be diagnosed and treated by performing tests, urine chemistry tests, urine bacterial culture tests, and blood BUN and creatinine concentrations as needed.
• These tests are followed up again as needed even after a urinary tract infection and its symptoms have cleared up.
• Urinary tract infections are more likely to recur when there is a congenital or acquired anomaly in the kidney, ureter, bladder, urethra, etc., or some preceding disease.
• The degree of kidney scarring does not seem to be so severe. You can do another test at a later time by consulting your homeroom pediatrician.
• If you need any treatment for future fever, vomiting, diarrhea, growth delay, etc., it is very important to prioritize urinalysis to see if a urinary tract infection has recurred before treatment.
• At this age, you must get at least a second dose of the vaccine for DTaP, hepatitis B, polio, rotavirus infection, HIV, and pneumonia.
• Receive diagnosis and treatment at the Department of Pediatrics and Adolescents, and consult with us about these problems. [Parents should also be at least the half-doctors-Child and Family Nursing Encyclopedia]-Volume 2 Prevention of pediatric and adolescent diseases and safety accidents, Volume 3 Growth and development of newborns, infants, school-age and adolescent children-Growth and development of the relevant age, 1 month after birth A milestone in the development of children aged ~6 years. Volume 4 Breastfeeding, Breastfeeding, Reasons. Volume 5 Artificial nutrition, milk, baby food, vitamins, minerals, proteins, carbohydrates, fat.
• See Urinary Tract Infections, etc.
• If you have more questions, please contact us again. Thank you. Lee Sang-won dream
The following is an example of questions and answers for online pediatric and adolescent health counseling on “Urinary Tract Infection and Urine Bacteria Culture Test”.
Q&A. Urinary tract infection, urine bacterial culture test
Q.
• Hello… You are sending a letter like this again. It was said that germs appeared again. My child is just over two months old.
My children do not have twelve, and they eat milk well. However, it is said that germs come out when I keep doing a urine test. It is said to be a 3rd grade bacteria in the type of bacteria. So, if the bacteria come out again in both urine tests this time, they take medicine and do another test.
I keep worrying. In this case, what are the symptoms of my child? I’m really worried. I eat well, but the germs keep coming out. The teacher said that the urine doesn’t come out clearly, but it seems to come out after being stagnated. I’ll have to do the test anyway. Teacher, what should I do.
• A
• Haengmi
• Good morning. Thanks for asking. That’s a good question. The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
• It takes considerable time and skill to get urine from children and adolescents to diagnose a urinary tract infection.
• Urine received in infant urine bags (pictures 1-34, 1-35) when stool was on the vulva, urine received without properly washing the exogenous organ, and urine blood sample left at room temperature for at least one or two hours after receiving , If a urine bacteriological test is performed with a urine sample received in a dirty container or a urine sample touched with a dirty hand, the test result may be abnormal.
• For this reason, if necessary, a urine catheter is inserted into the bladder through the urethra, and urine in the bladder is collected and a bacterial culture test is performed with the urine. Sometimes, urine in the bladder is directly drawn through the abdominal wall with a needle to cultivate urine bacteria. Do the test.
• When there is a urinary tract infection, the urine bacterial culture test result may appear abnormal. If a urine chemistry test is performed with the urine sample used for the bacterial culture test, abnormally many white blood cells and red blood cells may come out, and abnormally many bacteria. It is common to have.
• In other words, when you have a urinary tract infection, most of your urine chemistry test results are abnormal.
• I would like to know how you received your urine and tested it for urine bacteria, how the urine chemistry test resulted, and how the test result came out when your urine was examined under a microscope.
• There is only about 60% chance of having a urinary tract infection before starting antibiotic treatment, when the results of the first bacterium culture test are abnormal,
• When the secondary bacterial culture test results are abnormal, the probability of having a urinary tract infection is about 90%.
• When the third bacterial culture test results in abnormalities in all of the 1st, 2nd, and 3rd results, the probability of having a urinary tract infection is about 98%.
• For this reason, for infants and toddlers, it is difficult to confirm the presence of a urinary tract infection with a single urine bacterial culture test.
• Urine bacterial culture test and urine chemistry test with urine obtained with a needle (inhalation of upper pubic urine). If the test result is abnormal, kidney/ureter of the kidney or ureter by using renal ureteral ultrasonography, urinary ureterography, DMSA kidney scan, etc.
• Let’s find out if there are congenital malformations in the bladder or urethra, and to what extent the kidneys or ureters are damaged due to urinary tract infection.
• You do not have to do all of these tests at any time. However, if you do not do a renal ureteral ultrasonography, urinary ureterography, or DMSA kidney scan again, it would be a good idea to do it.
• Even if the results of the first urine bacterial culture are normal, it may be a good idea to do at least one more follow-up.
• Depending on the results of a urine bacterial culture test, you may also consider treating or preventing a urinary tract infection for at least 6 months to a year with appropriate antibiotics.
• As you may know, there are times when you consult a urologist for treatment in this case, but I think it is better to consult a pediatric nephrologist for treatment.
• Even with these treatments, I would like to tell you that the diagnosis and treatment methods are different depending on the situation at that time.
• See Urinary Tract Infection.
• If you have more questions, please contact us again. Thank you. Lee Sang-won .MD
The following is an example of questions and answers for online pediatric health counseling on “Urinary Tract Infection, Urine Bacteria Culture Test, and Consultation After Counseling”.
Q&A.
Urinary tract infection, urine bacterial culture test, consultation after consultation
Q.
• This morning, I received a note from the local Pediatrics Department and went to the general hospital, and the teacher said that it was not enough to go to a large hospital. My child says it is not a urinary tract infection.
• The teacher said that blood cells are mixed in urine, but it is still in the stage of observation.
• He said that there is a person in the family that is genetically such that it may be, and he said that he should watch for about 6 months.
• From a mother’s point of view, it’s not cool.
• A teacher who specializes in otorhinolaryngology saw her and said that her throat is swollen so much that she can have a high fever.
• She has been receiving throat pills and antipyretic drugs.
• On the teacher’s homepage, I read 1. My child’s sickness 1. Genitourinary disorders (hematuria). In the case of my child, it looks like latent hematuria. • Could there be many reasons for latent hematuria? Shouldn’t it be a quick and detailed inspection?
• Can you tell if it’s harmless hematuria just from a urine test done at the Pediatrics Department?
• A.
Dear Mihwa • Thank you for asking another question.
• I know you’ll be confused a lot by now. I am also confused a lot.
• I was afraid because I thought this would lead to confusion if I had health counseling over the Internet.
• He gave me the information, “I heard that my urine was mixed with blood, my stomach ache, and I urinate often, so I went to the hospital and it was cystitis”.
• The Department of Pediatrics and Adolescents told me that instead of diagnosing “I have cystitis,” they use the name “urinary tract infection” more.
• That is, I was told that my child had a urinary tract infection. “If a child has a history of urinary tract infections, they are more likely to get another urinary tract infection.”
• Urinalysis and Urine culture for bacteria are not 100% diagnosed as having a urinary tract infection because 100% of the results are abnormal.
• However, if there are signs of symptoms and the results of the urine test and urine culture are abnormal (100,000 or more colonies of the same type of bacteria), you may have a urinary tract infection.
• In other words, it means that it cannot be confirmed that your child had a urinary tract infection at the time.
• Because even when a 33-month-old girl’s exogenous tract is inflamed, it can be painful when urinating, it can be difficult to urinate frequently, and urine can have pyuria and hematuria.
• Also, when you receive urine for a blood sample for a urine bacterial culture test, a very small amount of feces may get into your urine. When a urine bacterial culture test is performed with such urine, the bacteria grown on the bacterial culture test may be erroneously determined to be bacteria from the kidney or bladder.
• For this reason, when diagnosing urinary tract infections in young infants and toddlers, rather than diagnosing urinary tract infections by receiving urine only once before starting antibiotic treatment and performing a urine bacterial culture test, sometimes two or three urine tests are performed. Urine bacterial culture tests may also be done two or three times.
• Sometimes the urine test results are normal, but you may have a urinary tract infection, and you may not have a urinary tract infection even though the urine bacterial culture test results are abnormal.
• Telling you more can get more complicated.
• There are many causes of latent blood in the urine.
• Urinary tract allergies, viral urinary tract infections, tuberculous urinary tract infections, kidney bruises, glomerulonephritis, physical exercise, bacterial urinary tract infections, allergic diseases, hypercalcemia, tumors, parasites, urinary tract foreign bodies, bleeding diseases, etc. Hematuria can occur for many reasons.
• You may only have hematuria even though your body is fine. This hematuria is called benign latent hematuria.
• Hematuria is getting worse day by day, or when latent hematuria is measured with a multistick chemistry test, the test results range from 1+ to 4+. The causes and diagnosis and treatment methods differ depending on the number of (+).
• Diagnosis and cause treatment are different depending on whether only hematuria, hematuria and proteinuria, or both hematuria and pyuria are present.
• In summary, there are many causes of hematuria, and it is sometimes difficult to pinpoint the cause of hematuria.
• It is said that the tonsils are swollen and have a fever, so I believe that everything has been recovered.
• If tonsillitis is caused by group A beta hemolytic streptococcus, glomerulonephritis should also be suspected. There is also febrile hematuria caused by fever.
• You may have a urinary tract infection, such as cystitis, without any malformation of the urinary system.
• Because you currently have hematuria, you may be wondering if it is related to hematuria and the first urinary tract infection you had.
• Also, it cannot be 100% ruled out that there is nothing wrong with the urinary system.
• Some doctors argue that it is a good idea to find out if you have a urinary tract infection because of any abnormalities or predecessors in the urinary system, even if you have a single urinary tract infection.
• It’s very complicated.
• If my child is my daughter, I will have a kidney, ureter, and bladder ultrasound in 2 to 3 weeks. In addition, urine is well collected, a urine test and a urine bacterial culture test are performed, and if the test result is normal and there is (+) blood in the urine, observation treatment will be performed without worrying.
• However, if there is more (+) blood in the urine and the results of other tests are abnormal, we will actively test for any abnormalities in the urinary system
. • Please consult with the Department of Pediatrics and Adolescents after receiving re-examination, diagnosis, and treatment.
• Sorry to confuse you.
• If you have more questions, please visit again.
• Thank you. Lee Sang-won .MD
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com 제7권 소아청소년 감염병
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, harvey grant and robert murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies , Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Berverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gerhon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD, FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”