영아 돌연사 증후군 직전 상태, Near-sudden infant death syndrome(Near-SIDS/near-miss sudden infant death syndrome)
영아 돌연사 증후군 직전 상태의 개요 및 증상 징후
-
숨을 비정상적으로 가쁘게 쉬기도 하고 20초 동안, 또는 20초 이상 동안 숨을 쉬지 않으면 무호흡(Apnea) 상태“라고 정의한다.
-
영아가 무호흡 상태에 빠지면 얼굴이 창백해지고, 드물게는 얼굴이 홍조 색으로 변할 수 있고, 근육의 힘이 쭉 빠지고 거의 질식 상태에 이를 수 있고, 그 다음으로는 영아 돌연사 직전 상태에 빠질 수도 있다.
-
그렇지만 영아 돌연사 증후군과 같이 급사하지 않고 살아 있고 무호흡 상태로 있는 징후를 “영아 돌연사 증후군(Near-sudden infant death syndrome/Near-SIDS) 직전 상태” 또는 거의 직전 영아 돌연사 증후군이라고 한다.
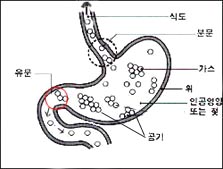
그림 410. 분문이 열려있다. 이때 위 식도 역류가 생길 수 있고 영아 돌연사 증후군 직전 상태까지 갈 수 있다. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
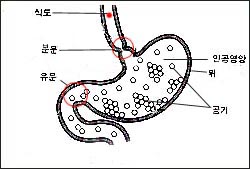
그림 409. 분문이 닫혀있다. 이때 위 식도 역류가 덜 생길 수 있고 영아 돌연사 증후군 직전 상태가 덜 생길 수 있다. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
-
이와 같이 영아가 영아 돌연사 증후군 직전 상태의 원인의 대부분은 확실히 모른다.
영아 돌연사 증후군 직전 상태의 진단 치료
-
신생아나 영유아가 적어도 20초 동안, 또는 그 이상 동안 숨을 쉬지 않는 상태를 “무호흡증(無呼吸症)” 또는 “무호흡 상태“라고 한다.
-
무호흡증의 원인이나 “영아 돌연사 증후군 직전 상태“의 원인을 알아보기 위해 자세한 병력, 세밀한 검진과 여러 가지 임상 검사를 해야 할 때가 많다.
-
피 검사, 가슴 X선 사진, 뇌 CT 스캔 검사, 바륨을 먹이면서 찍는 인두, 식도와 위 X선 사진, 심전도 검사, 뇌파검사, 뉴우모그래프 검사(Pneumography) 등으로 무호흡증의 원인이 무엇인지 알아보기도 한다.
-
감염병이나 신진대사 이상 등으로 무호흡증이 생길 수 있다. 그래서 그런 병이 있나 알아봐야 한다.
-
신생아나 영아에게 무호흡증이 있거나 “영아 돌연사 증후군 직전 상태“가 생기면 병원에 입원해서 심장박동, 호흡 상태, 혈압, 체온 등 인간 기본 생명유지 활력 징후 등이 정상인가 자세히 알아보고 심전도, 무호흡증 모니터, 뉴우모그래프의 검사를 하고 여러 날 동안 관찰하면서 무호흡증의 원인을 찾아 치료할 수 있다.
-
때로는, “무호흡증 모니터“로 여러 주 동안 집에서 추적 관찰을 할 수도 있지만 이런 관찰 치료의 가치에 관해 찬반론이 많다.
-
위식도 역류(胃食道逆流)이나 분문이완증(噴門弛緩症/Chalasia) 등으로 무호흡증이 생길 수 있고 영아가 돌연사 증후군 직전 상태로 갈 수 있다.[부모도 반의사가 되어야 한다–소아가정간호백과]-제9권 소아청소년 소화기계 질환–모유나 인공영양을 넘길 때 참조)
-
위식도 역류나 분문이완증을 적절히 치료해야한다.
-
위식도 역류나 분문이완증의 중증도가 심해서 무호흡증이 자주 생기면 음식물을 먹은 후 적어도 30∼60분 동안 영아 운반의자(Baby carrier)에 영아를 비스듬히 앉혀 위 속 음식물이 식도관 내로 역류되지 않도록 예방 치료를 하고 적절한 약물로 치료한다. 영아 운반의자에 영아를 비스듬히 앉혀 위 속 음식물이 식도관 내로 역류되지 않게 치료하는 방법에 대해서도 최근 찬반론이 있다.
-
무호흡증이 완전히 없어질 때까지 수 주 내지 수개월 동안 위에서 설명한 치료를 계속 할 때도 있다.
-
심한 위식도 역류는 분문 수술로 치료 한다.
영아 돌연사 증후군 직전 상태의 합병증
-
폐부종,
-
흡인성 폐렴,
-
중추신경 저산소증,
-
전신 경련 등
[부모도 반의사가 되어야 한다–소아가정간호백과]-제22권 아들 딸 이렇게 사랑해 키우세요
충분한 수면, 신생아의 잠, 태아, 신생아, 어린 자녀의 사망과 부모 참조.
Near-sudden infant death syndrome(Near-SIDS/near-miss sudden infant death syndrome)영아 돌연사 증후군 직전 상태
Overview of conditions immediately before Sudden Infant Death Syndrome and symptoms and signs
- If your child breathes abnormally quickly and does not breathe for 20 seconds or more than 20 seconds, it is defined as “Apnea”.
- When an infant falls into apnea, the face may become pale, and in rare cases, the face may turn red, muscle strength may drop out and almost suffocate, and then the infant may fall into a state on the verge of sudden death.
- However, signs of alive and apnea without sudden death, such as sudden infant death syndrome, are referred to as “near-sudden infant death syndrome (Near-SIDS) immediate pre-condition” or almost immediately preceding sudden infant death syndrome.
Figure 410. The cardiac sphincter is open. At this time, gastroesophageal reflux may occur and may go to a state just before sudden infant death syndrome. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 409. The cardiac sphincter is closed. At this time, gastroesophageal reflux may occur less and the condition immediately before sudden infant death syndrome may occur less. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
As such, most of the causes of the immediate pre-infant sudden infant death syndrome are not known for certain.
Diagnosis treatment of the condition immediately before sudden infant death syndrome
- A condition in which a newborn or infant does not breathe for at least 20 seconds or longer is called “apnea” or “apnea state”.
- A detailed medical history, detailed examination, and various clinical tests are often required to determine the cause of apnea or the cause of the “sudden infant death syndrome”.
- Find out what causes apnea using blood tests, chest X-rays, brain CT scans, pharynx taken while feeding barium, esophagus and stomach X-rays, electrocardiogram, electroencephalography, and pneumography also do.
- Apnea can occur due to infectious diseases or metabolic abnormalities. So you have to find out if you have such a disease.
- If a newborn or infant has apnea or has a “sudden infant death syndrome”, enter a hospital to find out in detail whether basic human vital signs such as heart rate, respiratory status, blood pressure, and body temperature are normal, electrocardiogram, apnea monitor, pneumograph
- You can find and treat the cause of apnea by doing the test for several days and observing it for several days. Sometimes, you can follow up at home for several weeks with “Apnea Monitor”, but there are many pros and cons about the value of such observational treatment.
- Apnea may occur due to gastroesophageal reflux (胃食道逆流) or cardioplegia (Chalasia), and infants may go to a state just before sudden death syndrome. Volume 9 Children and Adolescents Digestive System Diseases-Refer to the case of passing over breast milk or artificial nutrition) Gastroesophageal reflux or laxatives should be treated appropriately.
- If apnea occurs frequently due to severe gastroesophageal reflux, preventive treatment to prevent reflux of food in the stomach into the esophageal canal by placing the infant at an angle in a baby carrier for at least 30-60 minutes after eating food.
- Treat with appropriate medication.
- There are also recent pros and cons about how to treat an infant so that the food in the stomach does not flow back into the esophagus by seating the infant at an angle in the infant carrier chair.
- Sometimes the treatment described above is continued for weeks to months until the apnea is completely cleared.
- Severe gastroesophageal reflux is treated with cardiovascular surgery.
Complications immediately before sudden infant death syndrome
1. Pulmonary edema,
2. Aspiration pneumonia,
3. Central nervous system hypoxia,
4. General convulsions, etc.
- [Parents should also be at least the half-doctors-Pediatric Family Nursing Encyclopedia]-Book 22, love your sons and daughters like this
- See adequate sleep, the sleep of newborns, fetus, death of newborns, and young children and parents
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
Manual of emergency pediatrics 4th edition, Robert M. Reece, M.D., p.162-165
Emergency Pediatrics, A guide to ambulatory care, 5th edi. Roger M. Barkin, Peter Rosen, p.187-188
Quick Reference to Pediatric Emergencies, Delmer J. Pascoe, M.D., Mose Grossman, M.D., p.75-176
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.617, 619
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
Emergency care, Harvey grant, and Robert Murray
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
Manual of Emergency Care
응급환자관리 정담미디어
소아가정간호백과-부모도 반의사가 되어야 한다, 이상원 저
The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
Preparation for Birth. Beverly Savage and Dianna Smith
임신에서 신생아 돌보기까지. 이상원
Breastfeeding. by Ruth Lawrence and Robert Lawrence
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
Red book 29th-31st edition 2012
Nelson Text Book of Pediatrics 19th-21st Edition
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
The Harriet Lane Handbook 19th Edition
Growth and Development of Children, George H. Lowrey 8th edition
소아과학 대한교과서
제1권 소아청소년 응급의료 참조문헌과 출처
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”