심방 중격 결손 Atrial septal defect
심방 중격 결손의 개요
-
좌심방과 우심방을 나누는 막을 심방 중격이라고 하고
-
그 심방 중격의 결손으로 인해 생겨 있는 구멍을 심방 중격 결손이라 하고
-
그로 인해서 생기는 증상을 심방 중격 결손증이라고 한다.
-
심방 중격 결손증에는
- 난원공 개존,
- 2차공 심방 중격 결손,
- 심내막상 결손 3종류가 있다.
-
다음은 따로따로 설명한다.
심방 중격 결손의 종류
-
심방 중격 결손은
- 난원공 개존,
- 2차공 결손(2차공 심방 중격 결손),
- 심내막상 결손으로 크게 3분 된다.
-
태아기에는 우심방 속 모든 혈액이 삼천판을 통과한 후 우심실 속을 거쳐 폐로 흘러갈 필요가 없기 때문에 우심방 속 혈액의 일부가 정상적으로 좌심방 속으로 흘러가게 된다. 그럴 때 난원공 개존이 필요하다.
-
태어나기 전 모든 태아들의 심방 중격에 난원공이 정상적으로 뚫려 있다.
-
난원공을 심방 중격 결손증이라고 하지 않는다.
-
대부분의 난원공은 출생 후 바로 자연히 막히는 것이 정상이다.
-
그렇지만 드물게, 출생 후부터 죽을 때까지 난원공이 그대로 뚫려 있을 수 있다.
-
난원공의 크기는 바늘 하나가 들어갈 수 있을 정도이거나 그 보다 좀 더 클 수 있다(그림 10 참조). 이런 상태의 난원공을 난원공 개존 이라고 한다. 난원공 개존으로 인해 일생동안 아무런 증상 징후도 생기지 않고 일상 동안 생활 하는데 아무 지장를 주지 않는 것이 보통이다.
-
그러나 심방 중격에 있는 난원공 개존 이외 비정상적으로 심방 중격 결손증이 생겨 그로 인해 심방 중격에 비정상적으로 구멍이 크게 뚫려 있을 수 있다.
-
이것을 심방 중격 결손증이라고 한다.
-
심방 중격 결손증이 심방 중격의 어느 부위에 있느냐에 따라 심방 결손증은 여러 종류가 있을 수 있다.
심방 중격 결손의 심장 내 혈액 순환
-
정상 심장에서는, 좌심방 속 혈압은 우심방 속의 혈압보다 조금 더 높은 것이 정상이다.
-
큰 심방 중격 결손증이 있을 때는 다음과 같이 심장내 혈액 순환이 이루어진다.
-
좌심방 속 동맥혈의 일부가 심방 중격 결손 구멍을 통과해서 우심방 속으로 흘러 들어간다.
-
대정맥을 통해 전신에서 우심방 속으로 흘러 돌아온 정맥혈이 심방 중격 결손을 통해 들어온 동맥혈과 좌심방 속에서 섞이게 된다.
-
동맥혈과 정맥혈이 우심방 속에서 섞인 동맥 정맥 혼합 혈이 삼첨판을 통과해서 우심실 속으로 흘러 들어간다.
-
그 다음, 동맥혈 정맥혈이 섞인 우심실 속 동맥·정맥 혼합 혈은 폐동맥을 통과해서 폐 속으로 흘러 들어가게 된다.
-
이 때, 대정맥에서 우심방 속으로 흘러 들어온 정맥혈과 좌심방 속에서 우심방 속으로 흘러 들어온 동맥혈이 합친 동맥·정맥 혼합 혈이 다량으로 폐동맥 속을 통과해서 폐 속으로 들어가기 때문에 폐는 정상 이상으로 더 많은 혈액 양을 취급해야 한다.
-
이런저런 이유로, 좌심방, 우심방과 우심실이 보통 이상으로 일을 더 많이 해야 한다.
-
그 때문에 심장이 전체적으로 비정상적으로 더 커질 수 있다.
-
그래서 심장 전체가 비대해진다.
-
심장이 커지는 정도는 심방 중격 결손증의 크기와 종류에 따라 다르다.
-
생후 얼마 동안 심방 중격 결손증으로 심장이 비정상적으로 더 많이 커지지 않는 것이 보통이지만, 환아가 점점 더 자라면서 심장도 점차로 더 커질 수 있다.
심방 중격 결손의 증상 징후
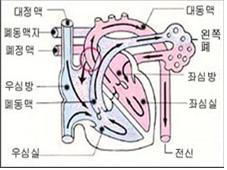
그림28. 심박 중격 결손증
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
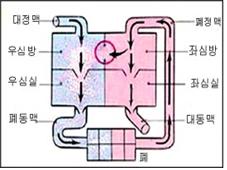
그림27. 심박 중격 결손증
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
-
심방 중격 결손증이 있는 환아의 나이, 심방 중격 결손 구멍의 크기, 다른 종류의 공존 선천성 심장혈관 질환 기형의 유무 등에 따라 증상 징후가 다르다.
-
공존 심장혈관 질환이 없이 작은 심방 중격 결손 구멍이 있을 때는 증상 징후가 거의 없는 것이 보통이다.
-
아주 큰 심방 중격 결손 구멍을 가진 아이에게 폐렴이 자주 생길 수 있다.
-
소아 건강검진을 주기적으로 받을 때 의사가 심잡음을 듣고 심방 중격 결손 구멍이 있다는 것을 우연히 진단할 때도 있다.
-
그러나 큰 심방 중격 결손 구멍이 있는 것을 평소에 전혀 모르고 있다가 우연히 진단 받는 경우도 있다.
-
상당히 큰 심방 중격 결손 구멍을 가진 아이들의 대부분은 성장 발육이 지연되고 쉽게 피로를 느끼고 폐렴에 더 자주 걸려 심하게 앓을 수 있고 때로는 심장부전증(심부전증)이 생겨 심하게 앓을 수도 있다.
-
성인이 될 때까지 상당히 큰 심방 중격 결손 구멍을 적절히 치료하지 않으면 생명에도 위험하고 여러 가지 합병증이 생길 수 있다.
심방 중격 결손의 진단
-
병력, 증상 징후와 진찰소견 등을 종합해서 이 병이 의심되면 심전도 검사, 가슴 X선 사진 검사, 심초음파 검사, 심장 초음파 상, 심도자법 검사 등 여러 검사로 쉽게 확진할 수 있다.
-
아주 작은 심방 중격 결손구멍이 있을 때는 아무런 증상이 없기 때문에 심방중격 결손 구멍이 있는지 모르고 지내는 경우도 많다.
-
정기 건강검진을 받을 때 의사가 청진기로 비정상 심잡음을 듣고서 심방 중격 결손구멍을 처음으로 진단하는 경우도 흔하다.
심방 중격 결손의 치료
-
심방 중격 결손구멍이 작을 때는 아무 치료가 요하지 않는다.
-
큰 심방 중격 결손구멍은 선택적 심장 수술로 심방 중격 결손 구멍을 막아 주는 수술 치료를 해야 한다.
-
대개 유치원에 입학하기 전 선택적 수술 치료를 해주는 것이 보통이다.
-
작은 심방 중격 결손 구멍을 치료해 주는 심장 수술은 비교적 간단하다.
심방 중격 결손증 새 ASO 심장수술 치료방법
-
우심방과 좌심방을 사이에 있는 칸막이 벽을 심방 중격이라고 한다.
-
이 심방 중격에는 난원공이란 구멍이 태어나기 바로 전까지 정상적으로 있다. 또는 출생 후 얼마동안 정상적으로 계속 그대로 개존 해 있을 수 있다.
-
대부분의 난원공은 출생 후 몇 주 후부터는 자연적으로 막히는 것이 정상이다.
-
심방 중격의 일부분에 선천적으로 비정상적으로 크게 뚫린 심방 중격 구멍을 한개만 갖고 태어날 수도 있다.그 구멍을 심방 중격 결손이라고 한다.
-
그 심방 중격 결손 구멍의 크기와 그로 인해 생기는 증상 징후에 따라 심장 수술 치료를 하기도 하고 때로는 아무 치료 없이 일생동안 관찰적 치료를 할 수 있다.
-
1954년 이후 심방 중격 결손 치료는 주로 전신마취 하 심장 개방수술로 치료했었다.
-
그러나 1976년 이후 심방 중격 결손을 심장 개방수술로 치료하는 대신 피부층 피하 조직을 통해 심방 중격 결손 구멍을 막는 Amplatzer Septal Occluder(ASO) 수술치료 방법으로 치료하는 것이 보통이다.
-
미국에서 연간 약 4만 명의 신생아들이 선천성 심장 기형을 가지고 태어난다.
-
그 중 10%는 ASO 수술 치료방법으로 치료한다고 한다.
-
최근에 약 4000~5000명의 심방 중격 결손을 ASO 수술 치료법으로 치료해서 심장 수술 치료 프로그램 개가를 올렸다고 한다.
-
또 최근에 442예의 심방 중격 결손증을 ASO 수술 치료법으로 치료한 결과와 심장 개방수술 치료를 한 결과에 비교할 때 ASO 수술 치료방법의 치료효과는 더 좋았고 또 더 안전한 치료법이었고 합병증의 발생률이 아주 적은 것으로 나타났다
Atrial septal defect 심방 중격 결손
Overview of atrial septal defect
• The membrane dividing the left and right atrium is called the atrial septum.
• A hole created by a defect in the atrial septum is called an atrial septal defect.
• The resulting symptom is called atrial septal defect.
In atrial septal defect
o Opening of the ovarian cavity,
o Secondary atrial septal defect,
o There are 3 types of endocardial defects.
• The following will be explained separately. Types of atrial septal defect
Atrial septal defect
1. Opening of the ovarian cavity,
2. Secondary hole defect (secondary hole atrial septal defect),
3. It is largely 3 minutes due to endocardial defect.
• In the prenatal period, part of the blood in the right atrium normally flows into the left atrium because it is not necessary to pass all the blood in the right atrium to the lungs through the right ventricle after passing through the tricuspid valve. In such a case, the existence of the Nanwon Gong is necessary.
• Before birth, the atrial septum of all fetuses is normally punctured.
• The oval hole is not called an atrial septal defect.
• It is normal for most ovarian cavities to block naturally immediately after birth. • Nevertheless, in rare cases, the oval hole may remain open from birth to death.
• The size of the oval hole can be large enough to fit a single needle (see Figure 10). The oval hole in this state is called the opening of the oval hole. Due to the opening of the ovarian cavity, it is common that there are no symptoms or signs during the lifetime and do not interfere with daily life.
• However, in addition to the opening of the oval hole in the atrial septum, abnormal atrial septal defect may occur, resulting in an abnormally large hole in the atrial septum.
• This is called an atrial septal defect.
• There can be several types of atrial septal defects, depending on where the atrial septal defect is located in the atrial septum.
Blood circulation in the heart in an atrial septal defect
• In a normal heart, it is normal for the blood pressure in the left atrium to be slightly higher than the blood pressure in the right atrium.
• When you have a large atrial septal defect, blood circulation occurs in the heart as follows.
• Part of the arterial blood in the left atrium passes through the atrial septal defect hole and flows into the right atrium.
• Venous blood that flows back from the whole body through the vena cava into the right atrium is mixed in the left atrium with arterial blood that has entered through the atrial septal defect.
• Arterial and venous blood mixed in the right atrium passes through the tricuspid valve and flows into the right ventricle. • Then, arterial blood and venous blood mixed with arterial and venous blood in the right ventricle pass through the pulmonary artery and flow into the lungs.
• At this time, the arterial/venous mixed blood, which is the combination of venous blood flowing from the vena cava into the right atrium and arterial blood flowing into the right atrium from the left atrium, passes through the pulmonary artery in a large amount and enters the lungs. You have to deal with sheep.
• For one reason or another, the left atrium, right atrium and right ventricle have to work more than usual.
• This can cause the heart to become abnormally larger overall.
• So the whole heart becomes enlarged. • The degree to which the heart grows depends on the size and type of atrial septal defect.
• For some time after birth, it is common for the heart to not grow abnormally larger with an atrial septal defect, but as the child grows, the heart may gradually grow larger.
Symptoms signs of an atrial septal defect
Figure 28. Heart rate septal defect Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 27. Heart rate septal defect Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Symptoms differ depending on the age of the child with atrial septal defect, the size of the atrial septal defect hole, and the presence or absence of other types of coexisting congenital cardiovascular disease malformations.
• When there is a small atrial septal defect hole without coexisting cardiovascular disease, there are usually few signs of symptoms.
• Pneumonia can often develop in children with very large atrial septal defect holes.
• During periodic pediatric health checkups, doctors sometimes hear heart murmurs and accidentally diagnose the presence of an atrial septal defect hole.
• However, there are cases in which the diagnosis of a large atrial septal defect is caused by accidental diagnosis after not knowing at all.
• Most of the children with fairly large atrial septal defect holes have delayed growth and development, become easily fatigued, develop pneumonia more often, and become severely ill, sometimes with heart failure (heart failure).
• Until adulthood, if a fairly large atrial septal defect orifice is not properly treated, it is life-threatening and can lead to complications.
Diagnosis of atrial septal defect
• If the disease is suspected by taking the medical history, symptoms, signs, and examination findings together, it can be easily confirmed by various tests such as an electrocardiogram, chest X-ray, echocardiography, echocardiography, and cardiography.
• When there is a very small atrial septal defect, there are no symptoms, so many people don’t know if there is an atrial septal defect.
• It is common for doctors to diagnose an atrial septal defect for the first time after hearing abnormal heart murmurs with a stethoscope during regular medical checkups.
Treatment of atrial septal defect
• When the atrial septal defect is small, no treatment is required.
• Large atrial septal defects require surgical treatment to close the atrial septal defect through selective heart surgery.
• It is common to provide selective surgical treatment prior to entering kindergarten.
• Heart surgery to treat a small atrial septal defect hole is relatively simple.
Atrial Septal Defect New ASO Heart Surgery Treatment Method
• The partition wall between the right and left atrium is called the atrial septum.
• In this atrial septum, a hole called an oval hole is normally present just before birth. Or, it may continue to exist normally for some time after birth.
• It is normal for most ovarian cavities to block spontaneously from a few weeks after birth.
• A person may be born with only one atrial septal hole, which is a congenital abnormally large opening in a portion of the atrial septum. That hole is called an atrial septal defect.
• Depending on the size of the atrial septal defect orifice and the symptoms it causes, cardiac surgery may be performed, sometimes with life-long observational treatment without any treatment.
• Since 1954, the treatment of atrial septal defects has been mainly treated with open heart surgery under general anesthesia.
• However, since 1976, instead of treating atrial septal defects with open heart surgery, it is common to treat them with Amplatzer Septal Occluder (ASO) surgery, which blocks the atrial septal defect through the subcutaneous tissue of the skin layer.
• About 40,000 newborns are born annually in the United States with congenital heart anomalies.
• Of those, 10% are said to be treated with ASO surgical treatment. • Recently, about 4000 to 5000 patients with atrial septal defects were treated with ASO surgical treatment, raising the price of the heart surgery treatment program.
• In addition, compared to the results of ASO surgical treatment and open heart surgery for 442 cases of atrial septal defects recently, the treatment effect of ASO surgery was better and safer, and the incidence of complications was very low. appear
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제7권 소아청소년 감염병
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”