신증후군(네프로시스 증후군) Nephrotic syndrome

사진 1-74. 소변에 단백이 있는지 알아보기 위해 멀티스틱스 소변 화학 검사를 하면, 2~5분 내에 결과를 알 수 있다.
Copyrightⓒ 2011 John Sangwon Lee,MD., FAAP
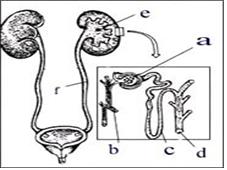
그림 1-73. 사구체에 생긴 신증후군으로 소변에 다량의 단백질이 분비될 수 있다.
a-사구체, b-동맥 혈관, c-신요세관, d-신요세관의 한쪽 끝이 신배로 연결된다. e-신우, f-요관. Copyrightⓒ 2011 John Sangwon Lee,MD., FAAP
다음과 같은 특이한 생화학적 변화가 체내에 생기는 신장병을 네프로시스 증후군 또는 신증후군이라고 한다.
- 소변에 단백이 비정상적으로 많이 나온다.(단백뇨)
- 소변에 단백이 비정상적으로 많이 나오기 때문에, 혈 중 단백 농도가 정상 이하로 감소된다.(저단백혈증)
- 신장 사구체 손상으로 소변이 정상적으로 분비되지 못한다.(감요증)
- 저단백혈증으로 전신에 수분이 비정상적으로 많이 괴어 전신이 붓는다.(부종)
- 핏 속 지방이 비정상적으로 많이 증가하여 혈중 지방 농도가 높다.(고지방혈증)
- 그 외 (그림 참조)
신증후군(네프로시스 증후군)의 원인
- 신증후군은 1차성 신증후군(원발성 신증후군)과 2차성 신증후군으로 구분된다.
- 1차성 신증후군의 원인은 아직 확실히 모른다.
- 몸에 다른 병이 없이 신장에만 병변이 생겨 신증후군이 생길 때 1차성 신증후군이라 하고,
- 신체의 다른 계통의 어떤 장기에 있는 병으로 생긴 신증후군을 2차성 신증후군이라고 한다.
- 2차성 신증후군은 벌 알레르기, 약물 중독, 옻 알레르기, 당뇨병, 헤노흐-쇤라인 자반증, 전신 홍반성 낭창, 또는 간염이나 매독 등으로 2차성 신증후군이 생길 수 있다.
- 여기서는 1차성 신증후군에 대해서 주로 설명한다.
- 1차성 신증후군이 발생되기 4∼8일 전에 감기나 그 외 다른 종류의 바이러스 상기도염 등을 앓았던 병력이 있는 경우가 많다.
- 그래서 감기 등 상기도 바이러스 감염병을 일으킨 바이러스의 항원 항체 이상반응으로 이 병이 생기는 것으로 추정된다.
- 또 이 병이 있는 환아의 친 부모 형제자매에게 이 병을 앓았던 가족 병력이 있을 수 있기 때문에, 유전성이 있다고 본다.
- 이 병이 있으면, 사구체의 기저막에 손상이 생기고, 그로 인해 사구체가 피를 정상적으로 여과하지 못한다.
- 사구체의 기저막 손상으로 혈 중 단백이 많이 여과되어, 소변에 단백이 비정상적으로 많이 나온다.
- 이 병은 생후 6개월 이전 신생아들, 영아들에게는 드물게 발생되지만, 2∼7세 연령층 남 유아들 또는 학령기 아이들에게 더 잘 발생된다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제15권 소아청소년 알레르기 및 면역질환-벌에 쏘였을 때, 혈청병, 약물에 의한 신장염
신증후군(네프로시스 증후군)의 증상 징후
- 여기서는 주로 1차성 신증후군의 전형적인 증상에 관해 설명한다.
- 이 병이 생기면 얼굴·몸·팔·다리·배·외음부 등이 붓고, 폐와 복강 내에 체액이 고여 복수가 차고, 늑막강(흉막강)에도 체액이 고이고 폐에 체액이 차서 숨이 가빠질 수 있다.
- 소변이 신장에서 정상적으로 분비되지 않기 때문에, 소변을 누어도 거의 나오지 않거나 아주 조금 나올 수 있다.
- 전신에 부종이 생겨 체중이 비정상적으로 증가된다.
- 식욕이 없고, 몸이 피곤하다. 급성 사구체 신염을 앓을 때처럼 고혈압은 거의 생기지 않는다.
- 이런 여러 증상 징후가 나타나지만, 많이 아픈 아이같이 보이지 않는 것이 보통이다.
- 혈 중 단백 농도가 비정상적으로 낮고, 전신에 생긴 부종, 그 외 여러 가지 이유로 박테리아, 바이러스 또는 다른 병원체에 쉽게 감염될 수 있다. 그래서 패혈증·폐렴·복막염·골수염 등 생명에 위험한 박테리아 감염병이 합병증으로 생길 수 있다.
- 또 신증후군 치료에 주로 쓰는 코르티코스테로이드제로 면역 체계 기능이 감소될 수도 있고, 그로 인해 박테리아, 바이러스 또는 그 외 다른 병원체의 감염에 대한 저항력이 비정상적으로 약해질 수 있다.
- 이 병을 앓는 동안, 박테리아 감염이나 바이러스 감염성 감염병에 걸릴 가능성이 대단히 많다.
- 이 병을 앓을 때 미열이 나든지 고열이 나든지, 의사의 진단치료를 속히 받아야 한다.
- 신증후군을 앓을 때 열이 나면, 집중 치료실에서 치료 받는 것이 보통이다.
신증후군(네프로시스 증후군)의 진단과 감별 진단
- 병력·증상 징후·진찰소견 등을 종합하여 이 병이 의심되면, 소변검사, 소변 화학 검사, 피검사 등으로 진단한다.
- 소변에 단백이 비정상적으로 많이 나오고, 혈 중 단백 농도가 비정상적으로 낮고, 혈중 지방의 농도가 비정상적으로 높으면 이 병을 진단할 수 있다.
- 24시간 동안 받은 총 소변으로 여러 종류의 소변검사를 해서 진단하는 데 도움을 얻는다.
- 때로는 신장 생체 조직 검사로 이 병을 확진한다.
- A군 베타 용혈성 연쇄상구균 감염 후 생기는 급성 사구체 신염, 그 외 사구체 신염, 급성 아나필락시스 자반증, 약물 알레르기성 신증후군이나 옻 알레르기 신증후군 또는 벌 알레르기 신증후군 등과 감별 진단해야 한다.
신증후군(네프로시스 증후군)의 치료
- 이 병의 중증도, 병일, 합병증의 유무 등에 따라 치료가 다르다.
- 이 병이 의심되면 집중 치료실에 입원해서 진단·치료해야 한다.
- 프레드니손(체중 kg당 2mg을 1일 총 용량으로 계산해서)제로 단백뇨가 더 이상 소변에서 나오지 않을 때까지 치료하는 것이 보통이다.
- 프레드니손제로 치료 받기 시작해서 소변에 단백이 더 이상 나오지 않을 때까지의 기간은 대략 10∼14일이다.
- 소변에 단백이 더 이상 나오지 않으면 프레드니손제의 용량을 점차로 줄이다가 마지막에 아주 끊는 식으로 치료한다. 이런 식으로 치료를 시작한 지 4주 정도에 환아들의 90% 정도는 완전히 회복되는 것이 보통이다.
- 환아들 중 5% 정도는 2주 정도 프레드니손제로 치료하면 비로소 치료 효과가 나타나기 시작할 수 있다. 일부 환아는 치료 시작한 지 3, 4일에 치료 효과가 나타날 수 있다.
- 그러나 환아 중 10%는 프레드니손제 치료를 2개월 동안 계속 한 후에야 비로소 치료 효과가 나타나기 시작한다.
- 프레드니손제로 2개월 동안 치료한 후에도 치료 효과가 뚜렷하게 나타나지 않으면, 프레드니손제 치료를 더 이상 하지 말고 사이클로포스파마이드나 다른 종류의 약으로 치료하는 것이 보통이다.
- 이 병을 초기에 치료할 때 식염과 수분 섭취를 적절히 제한하다가, 병세가 호전되면서 평소에 먹던 음식물로 점차로 바꾸어 준다.
- 이 병을 앓을 때, 될 수 있는 한 환아의 기력에 따라 육체적 활동량을 적절히 조절하는 것이 좋다.
- 복강 내, 늑막강(흉막강) 내 또는 신체의 다른 계통의 장기와 조직에 체액이 비정상적으로 많이 고일 수 있다. 그러나 체액을 주사바늘로 빼내는 치료를 해서는 안 된다.
- 신체의 거의 모든 장기와 조직에 비정상적으로 고여 있는 체액은, 이 병이 다 나으면 자연적으로 전부 빠지고, 복강 내 체액도 자연히 빠진다.
- 이 병을 앓는 동안 감기나 다른 종류의 바이러스 호흡기 감염병이나 박테리아 감염병에 걸리기 쉽기 때문에, 감염병을 앓는 사람에게 접근하거나 접촉하지 않도록 주의해야 한다.
- 특히 프레드니손제 또는 사이클로포스파마이드제로 치료를 받을 때 수두를 앓는 환아와 절대로 접촉하면 안 된다.
- 과거에 수두를 앓은 후 수두 면역이 있는 아이의 신증후군을 프레드니손제나 사이클로포스파마이드제로 치료받으면 수두 면역력이 감소되고 거기다가 신증후군으로 면역 기능이 약해지기 때문에 수두에 또 걸릴 수 있고, 일단 걸리면 생명이 위험할 정도로 심하게 앓을 수 있다.
- 일반적으로, 이 병의 예후는 좋은 편이지만, 환아의 10%는 사이클로포스파마이드제 치료나 그 외 치료를 몇 년 동안 계속받아야 할 때도 있다.
- 그 중 일부 환아 경우, 신장이 심하게 손상되어 약물치료를 적절히 받아도 치료 효과가 전혀 나타나지 않아 생명에도 위험할 수 있다.
- 프레드니손제 치료로 증상 징후가 전혀 없이 완화된 환아 중 30% 정도는 재발되지 않으나, 약 10% 정도는 재발될 수 있다.
- 병이 재발되면, 처음 발병됐을 때와 같이 다시 치료를 시작해야 한다.
- 이상 설명한 치료 방법은 환아에 따라, 병의 중증도에 따라, 합병증에 따라, 의사에 따라 그때그때 다를 수 있다.
|
다음은“신증후군의 식단”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q.&A. 신증후군의 식단에 대해
Q.
- 안녕하세요. 5살 남자 아이입니다.
- 미세 변화 신증후군이라는 진단을 받고 병원에서 퇴원을 했습니다.
- 식이요법을 하고 싶은데, 이런 병에 걸린 사이트를 찾아도 없고 해서 답답한 마음에 글을 올립니다.
- 또 신중후근의 전문 병원과 전문의도 함께 알려주시면 감사하겠습니다.
A.
- 현이 엄마께
- 안녕하십니까. 좋은 질문해 주셔서 감사합니다.
- 자녀의 나이와 성별, 과거·현재의 병력, 가족의 병력, 증상 징후와 진찰소견, 적절한 임상검사 등의 결과를 종합해서 진단·치료하는 것이 이상적이지만, 주신 정보를 참작해서 답변을 드립니다.
- 신증후군을 치료하는 식이요법은 병의 중증도와 병의 자연 진행시기에 따라 많이 다릅니다. 또 아이의 연령에 따라 다릅니다. 그리고 식성에 따라 많이 다릅니다.
- 부종이 있을 때 처음 얼마 동안은 “소금이나 간장을 가하지 않은 음식물“을 섭취하게 하고, 환아에게 줄 음식을 요리할 때 소금이나 간장을 넣지 않고 요리해야 합니다.
- 그리고 소금을 많이 가한 짠 음식물이나 과자 등을 환아 자신이 먹을 수 없도록 보관해야 합니다.
- 그러나 부종이 없어진 후에는, 음식물 종류와 분량에 제한 없이 먹여야 합니다. 부종이 아주 심하지 않는 한, 수분 섭취를 제한할 필요는 없습니다.
- 더 자세한 식이요법에 관해서는 담당 의사나 영양사에게 문의하시든지, 도서관이나 서점에서 참고서를 이용해서 참고하시기 바랍니다. 그리고 영양사의 조언을 받으면 좋을 것입니다.
- 신증후군을 참조하시기 바랍니다.
- 질문이 더 있으면, 또 방문하세요. 감사합니다. 이상원 드림
Nephrotic syndrome 신증후군
Photo 1-74. If you do a Multistick urine chemistry test to see if there is protein in your urine, you can get the results within 2 to 5 minutes. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 1-73. This is a nephrotic syndrome in the glomerulus that can secrete large amounts of protein in the urine. One end of the a-glomerular, b-arterial vessel, c-renal tubule, d-renal tubule is connected by a renal vessel. e-Shinwoo, f-ureter. Copyrightⓒ 2011 John Sangwon Lee, MD., FAAP
Nephrotic syndrome or nephrotic syndrome is a kidney disease in which the following peculiar biochemical changes occur in the body.
• Abnormally large amounts of protein in the urine (proteinuria).
• Since there is an abnormally large amount of protein in the urine, the level of protein in the blood decreases below normal (hypoproteinemia).
• Urine cannot be secreted normally due to damage to the renal glomerulus.
• Due to hypoproteinemia, the whole body is swollen due to abnormally large amounts of water (edema)
• The fat in the blood is abnormally increased and the fat concentration in the blood is high (hyperlipemia).
• Others (see picture)
Causes of nephrotic syndrome (nephrotic syndrome)
• Nephrotic syndrome is divided into primary nephrotic syndrome (primary nephrotic syndrome) and secondary nephrotic syndrome.
• The cause of primary nephrotic syndrome is still unknown.
• When nephrotic syndrome occurs due to lesions only in the kidneys without other diseases in the body, it is called primary nephrotic syndrome.
• Nephrotic syndrome caused by a disease in an organ in another system of the body is called secondary nephrotic syndrome.
• Secondary nephrotic syndrome can result from bee allergy, drug addiction, poison ivy allergy, diabetes, Henoch-Schoon’s purpura, systemic lupus erythematosus, or hepatitis or syphilis.
• Here, primary nephrotic syndrome is mainly explained. • There is often a history of having a cold or other types of viral upper respiratory tract infections 4 to 8 days before the onset of primary nephrotic syndrome.
• So, it is presumed that this disease is caused by an adverse reaction to the antigen antibody of the virus that caused the upper respiratory tract virus infectious disease, such as a cold.
• Also, since the child’s biological parents, siblings, and siblings may have a family history of the disease, it is considered hereditary.
• With this disease, damage to the basement membrane of the glomerulus is caused, which prevents the glomerulus from filtering blood normally.
• A lot of protein in the blood is filtered out due to damage to the basement membrane of the glomerulus, and abnormally a lot of protein comes out in the urine.
• The disease rarely occurs in newborns and infants before 6 months of age, but it is more common in boys aged 2 to 7 years or in school-age children. [Parents should also be anti-doctors-Child and Family Nursing Encyclopedia]-Vol. 15 Child and Adolescent Allergy and Immune Diseases-Nephritis caused by bee stings, serum diseases and drugs
Symptoms signs of nephrotic syndrome
• This section mainly describes the typical symptoms of primary nephrotic syndrome.
• When this disease occurs, the face, body, arms, legs, stomach, and vulva become swollen, fluid accumulates in the lungs and abdominal cavity, causing ascites, and fluid builds up in the pleural cavity (pleural cavity), and the lungs become filled with fluid, causing shortness of breath. I can.
• Because urine is not secreted normally by the kidneys, it may come out little or very little when you urinate.
• Body swelling causes abnormal weight gain.
• I have no appetite and my body is tired. High blood pressure rarely develops, as with acute glomerulonephritis.
• Many of these symptoms appear, but they usually don’t look like a very sick child.
• Abnormally low levels of protein in the blood, swelling of the body, and many other reasons are susceptible to infection by bacteria, viruses, or other pathogens. So, life-threatening bacterial infections such as sepsis, pneumonia, peritonitis, and osteomyelitis can occur as complications.
• In addition, corticosteroids used primarily to treat nephrotic syndrome may reduce immune system function, resulting in abnormally weakened resistance to infection by bacteria, viruses, or other pathogens.
• During this illness, you are very likely to get a bacterial or viral infection.
• Whether you have a mild or high fever when you have this disease, you should seek medical attention as soon as possible.
• If you have a fever while suffering from nephrotic syndrome, it is common to seek treatment in an intensive care unit.
Diagnosis and differential diagnosis of nephrotic syndrome (nephrotic syndrome)
• If this disease is suspected by taking the medical history, symptoms, and examination findings together, it is diagnosed with a urine test, a urine chemistry test, and a blood test.
• This disease can be diagnosed if there is an abnormally large amount of protein in the urine, the protein concentration in the blood is abnormally low, and the concentration of fat in the blood is abnormally high.
• Get help in diagnosing by doing several types of urine tests with total urine received over a 24-hour period.
• Sometimes a kidney biopsy confirms the disease.
• Acute glomerulonephritis, other glomerulonephritis, acute anaphylaxis purpura, drug allergic nephrotic syndrome, poison poison allergic nephrotic syndrome, or Bee allergic nephrotic syndrome, which occurs after group A beta hemolytic streptococcal infection, should be differentially diagnosed.
Treatment of nephrotic syndrome (nephrotic syndrome)
• Treatment differs depending on the severity of the disease, the day of the disease, and the presence or absence of complications.
• If you suspect this disease, you should be admitted to an intensive care unit for diagnosis and treatment.
• It is common to treat proteinuria with prednisone (2 mg per kilogram of body weight calculated as the total daily dose) until proteinuria is no longer coming out of the urine.
• The period from starting treatment with prednisone until the protein is no longer present in the urine is approximately 10-14 days.
• When the protein is no longer present in the urine, the dose of prednisone is gradually reduced, and then the treatment is stopped very much at the end. It is common for 90% of children to recover completely within 4 weeks of starting treatment in this way.
• About 5% of children are treated with prednisone for 2 weeks before the treatment begins to show effect. In some children, treatment effects may appear on the 3rd or 4th day of treatment.
• However, in 10% of children, the treatment effect begins to appear only after the treatment of prednisone is continued for 2 months.
• If treatment with prednisone is not evident after 2 months of treatment, it is common to stop prednisone treatment and treat with cyclophosphamide or another type of medication.
• When treating this disease at an early stage, adequately limit salt and fluid intake, and gradually change to the usual food as the condition improves.
• When suffering from this disease, it is advisable to properly adjust the amount of physical activity according to the patient’s energy as much as possible.
• Abnormal amounts of fluid may accumulate in the abdominal cavity, in the pleural cavity (pleural cavity), or in organs and tissues of other systems in the body. However, treatment that drains body fluids with an injection needle should not be performed.
• Abnormally accumulating fluids in almost all organs and tissues of the body naturally disappear when the disease is over, and fluids in the abdominal cavity also naturally drain.
• Because you are more susceptible to colds or other types of viral respiratory or bacterial infections while suffering from this disease, care should be taken not to approach or come into contact with anyone suffering from this disease.
• Never come into contact with a patient with chickenpox, especially when receiving treatment with prednisone or cyclophosphamide.
• If the kidney syndrome of a child who has chickenpox immunity after suffering from chickenpox in the past is treated with prednisone or cyclophosphamide, chickenpox immunity decreases and the immune function is weakened by nephrotic syndrome, so you may get chickenpox again. It can be so severely ill that life is dangerous.
• In general, the prognosis for this disease is good, but 10% of children may need cyclophosphamide treatment or other treatment for several years.
• In some cases, the kidneys are severely damaged, so even if they receive proper medication, the therapeutic effect does not appear at all, which can be dangerous to life.
• About 30% of children who are relieved with no symptoms of prednisone treatment do not recur, but about 10% may recur.
• If the disease recurs, treatment should be started again as in the first case. • The treatment methods described above may vary from time to time depending on the patient, the severity of the disease, complications, and doctors.
The following is an example of a question-and-answer for pediatric and adolescent health counseling on the Internet about the diet for nephrotic syndrome.
Q.&A.
About the diet for nephrotic syndrome Q.
• Good morning. This is a 5 year old boy.
• Was discharged from the hospital after being diagnosed with subtle change nephrotic syndrome.
• I want to diet, but I am frustrated because I haven’t been able to find a site with such a disease.
• In addition, I would appreciate it if you would inform us of the special hospital and specialists of Shin Joong Fu Geun.
A.
• Hyun to Mom
• Hello. Thanks for the great question.
• It is ideal to diagnose and treat the child’s age and gender, past and present medical history, family medical history, symptom signs and medical examination findings, and appropriate clinical tests. However, we will respond based on the information provided.
• The diet that treats nephrotic syndrome varies greatly depending on the severity of the disease and the natural progression of the disease. It also depends on the child’s age. And it depends a lot on diet.
• When you have swelling, make sure you eat “food without salt or soy sauce” for the first time, and when you cook food for your child, you should cook without salt or soy sauce.
• In addition, salty foods or snacks with a lot of salt should be stored so that they cannot be eaten by themselves.
• However, after the swelling has gone away, it should be fed without restrictions on the type and amount of food. Unless the swelling is very severe, there is no need to limit fluid intake.
• For more detailed diet information, ask your doctor or dietitian or use a reference book at the library or bookstore. And it would be nice to get advice from a nutritionist. • See Nephrotic Syndrome. • More questions
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Nelson Textbook of Pediatrics 14th ed. Beherman,
-
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th edition 2012
-
Nelson Text Book of Pediatrics 19th Edition
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gerhon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”