신생아 후비공 폐쇄(후비공 폐쇄/선천성 후비공 폐쇄) Choanal atresia of newborn infants
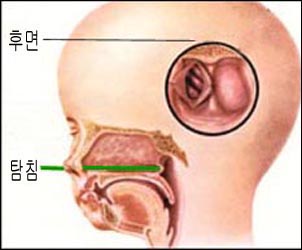
그림 104. 선천성 후비공 폐쇄.
a-탐침, b-비강 후면에서 본 선천성 후비공 폐쇄.
탐침 끝이 가리키고 있는 비강 후부에 선천성 후비공 폐쇄가 생겨 있다.
참조문헌; Used with permission from Clinical Educational Aid, Ross Labotories, Columbus, Ohio, USA와 소아가정의학백과
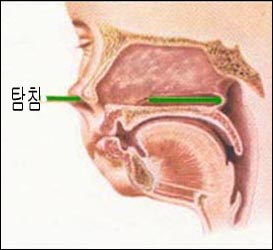
그림 104. 선천성 후비공 폐쇄.
a-탐침의 끝이 있는 후비공이 폐쇄되었다. b-탐침으로 후비공 폐쇄로 진단하고 있다.
출처; Used with permission from Clinical Educational Aid, Ross Labotories, Columbus, Ohio, USA와 소아가정의학백과
신생아 후비공 폐쇄의 개요
- 비강의 맨 뒤 부분을 후비공이라고 한다.
- 후비공은 비강의 맨 뒤에 있고 그 후비공은 인두 강으로 바로 연결된다.
- 후비공의 한쪽 또는 양쪽이 선천성으로 폐쇄될 수 있다.
- 양쪽 후비공 또는 한쪽 후비공이 전부 또는 일부가 폐쇄될 수 있고 후비공이 점막층으로 폐쇄될 수 있고 후비공이 뼈로 폐쇄될 수 있다.
- 이렇게 생긴 선천성 기형을 후비공 폐쇄, 선천성 후비공 폐쇄 또는 신생아 후비공 폐쇄라고 한다.
- 후비공이 선천성으로 폐쇄될 수 있고 후천성으로 폐쇄될 수 있다.
- 후비공이 후천성으로 폐쇄되면 후천성 후비공 폐쇄라고 한다.
후비공 폐쇄 종류
- 양측성 후비공 폐쇄,
- 일측성 후비공 폐쇄,
- 골성 후비공 폐쇄,
- 점막층성 후비공 폐쇄,
- 선천성 후비공 폐쇄,
- 후천선 후비공 폐쇄,
- 완전 골성 후비공 폐쇄,
- 양측성 골성 선천성 후비공 폐쇄, [부모도 반의사가 되어야 한다-소아가정간호백과]-제 3권 신생아, 영유아, 학령기와 사춘기 아이들의 성장발육-신생아의 코 참조.
후비공 폐쇄 발생률
- 신생아 후비공 폐쇄는 5000~7000 생존 신생아들 중 1명에게 생긴다(출처;Contemporary pediatrics, November 2008. p.38).
- 그 중 ⅔에서 한 쪽에만 생긴다.
- 남아들보다 여아들에게 더 잘 생긴다.
- 남여 발생 비율은 2:1이다.
- 왼쪽보다 오른쪽에 2배 더 생긴다.
- 후비공 폐쇄의 90%는 뼈로 막혀 생긴 골성 후비공 폐쇄이고
- 10%는 점막층으로 막혀 생긴 점막층성 후비공 폐쇄이다.
후비공 폐쇄와 공존이환(동반 질환)
- 신생아 후비공 폐쇄만 있는 신생아에게 다른 선천성 기형이 없이 생길 수 있고
- 안(눈)조직 결손증,
- 심장 기형,
- 지능 저하,
- 성장 지연,
- 생식기계 이상,
- 귀 이상 등 기형을 동반할 수 있고,
- 때로는 다운 증후군,
- 알펄트 증후군,
- 크로우존씨 병,
- 피에르 로빈 증후군 등의 드문 병과 동시 있을 수 있다.
- 그런 드문 병과 함께 생길 때가 더 많다.(출처;Contemporary pediatrics, November 2008. p.38).
후비공 폐쇄의 증상 징후
- 양쪽 후비공 폐쇄가 있는 선천성으로 갓 태어난 신생아는 코를 통해 숨을 전혀 쉴 수 없기 때문에 태어나자마자 심한 호흡곤란이 생기고 피부가 새파랗게 질릴 수 있고 전신성 청색증이 생길 수 있다.
- 이 기형이 한쪽 비강 후부에 있는 후비공에만 있을 때는 거의 정상적으로 숨 쉴 수도 있고 심한 호흡곤란이 생길 수도 있다.
- 심한 호흡곤란이 생기는 동시에 전신성 청색증도 생기는 것이 보통이다.
- 숨을 쉬려고 노력할 때 앞가슴이 흉강 속으로 빨려들어 가는 현상이 생길 수 있다.
- 아기가 우는 동안 입을 벌리고 입으로 숨을 쉴 수 있기 때문에 청색증이 일시적으로 없어지거나 덜 하는 것이 보통이다.
- 젖이나 인공영양을 제대로 빨아먹을 수가 없고 기본 생명유지를 하기가 대단히 위험한 기형이다.
후비공 폐쇄의 진단
- 콧구멍을 통해 비강 속에 가는 피딩 세관(Feeding tube)이나 탐침을 집어넣어 그 세관이 콧구멍과 비강 속을 통과한 후 후비공을 통과해서 인두강 속으로 나오는지 안 나오는지를 알아보는 검사로 이 기형을 진단하기도 한다(그림 101, 102 참조).
- 조영물을 콧구멍 속을 통해 비강 속에 넣고 조영물이 인두 강 상부 속으로 흘러나오나 알아보기 위해 코 X-선 사진을 찍어 진단할 수 있다.
- 그림 101, 102와 같이 탐침으로 진단할 수 있다.
- 벌브 주사기(Bulb syringe)로 콧구멍을 막을 때 숨 쉬는 공기로 벌브주사기 속이 차는지 알아 진단 할 수 있고,
- 고실계측계로 진단하기도 한다.
- 솜털을 얇고 가늘게 펴서 환아의 콧구멍 가까이에다 대고 솜털이 숨 쉬는 대로 콧구멍, 비강 등을 통해서 공기가 정상적으로 들어갔다 나왔다 하는지 알아보고 진단하든지
- 비강 CT 스캔 검사로 진단할 수 있다.
후비공 폐쇄의 치료
- 응급으로 치료한다.
- 입을 통해서 숨을 쉬게한다.
- 우선 경구 기도 관을 입안에 넣어주고 그를 통해 숨을 쉬게 하고 가능한 한 조기에 폐쇄된 후비공을 수술로 치료한다.
- 경구 기도 관을 입안에 삽입해 그 기도 관을 통해 숨 쉬게 치료하다가 적기에 선택적 수술 치료한다.
- 비공을 통해 수술하고 수술 결과는 일반적으로 좋다.
Choanal atresia of newborn infants 신생아 후비공 폐쇄(후비공 폐쇄/선천성 후비공 폐쇄)
Figure 104. Congenital Choanal atresia. a-probe, b-Choanal atresia viewed from the back of the nasal cavity. There is a congenital posterior nostril obstruction in the posterior nasal cavity where the tip of the probe is pointing. references; Used with permission from Clinical Educational Aid, Ross Laboratories, Columbus, Ohio, USA and the Encyclopedia of Pediatric and Family Medicine
Figure 104. Congenital Choanal atresia. The posterior nostril with the tip of the a-probe was closed. The b-probe is diagnosing Choanal atresia. source; Used with permission from Clinical Educational Aid, Ross Laboratories, Columbus, Ohio, USA and the Encyclopedia of Pediatric and Family Medicine
Overview of neonatal Choanal atresia
• The back part of the nasal cavity is called the Choana.
• The posterior nostril is at the back of the nasal cavity, which leads directly into the pharyngeal cavity.
• One or both of the posterior nostrils may be congenitally obstructed.
• Both orbital or unilateral posterior nostrils may be completely or partially occluded, the posterior nasal cavity may be occluded with a mucosal layer, and the posterior nasal cavity may be closed with bone.
• This congenital anomaly is called Choanal atresia.
• The posterior nostrils may be congenitally obstructed or acquired acquired. • Acquired nostril obstruction is called acquired nostril obstruction.
Types of Choanal atresia
• Bilateral Choanal atresia;
• Unilateral Choanal atresia;
• occlusion of the bony Choanal atresia;
• mucosal occlusion of the Choanal atresia;
• congenital Choanal atresia;
• Complete osseous Choanal atresia;
• Bilateral osseous congenital Choanal atresia,www.drleepediatrics.com – Volume 3 Growth and Development of Newborns, Infants, School-age and Adolescent Children – See Newborn Nose. Occurrence of posterior nostril obstruction
• Neonatal Choanal atresia occurs in 1 in 5000 to 7000 surviving newborns (Source; Contemporary pediatrics, November 2008. p.38).
• It occurs only on one side in two-thirds of them.
• It occurs more often in girls than in boys.
• The male to female ratio is 2:1.
• It occurs twice as often on the right side as on the left side.
• 90% of Choanal atresia are osseous occipital occlusions due to bone blockage
• 10% are mucosal Choanal atresia due to blockage of the mucosal layer. Occlusion and comorbidities (comorbidities)
• Newborns with only neonatal Choanal atresia can develop without other congenital anomalies and
• Eye (eye) tissue defects;
• heart malformations;
• Decreased intelligence;
• growth retardation;
• reproductive system abnormalities;
• It may be accompanied by deformities such as ear abnormalities,
• Sometimes Down’s syndrome;
• Alpert’s Syndrome;
• Crowe John’s disease;
• It may co-exist with rare diseases such as Pierre Robin syndrome.
• It is more common with such rare diseases (source; Contemporary pediatrics, November 2008. p.38).
Symptoms, signs of Choanal atresia
• Newborns born with congenital occlusion of both nostrils can develop severe dyspnea immediately after birth, their skin may turn blue, and systemic cyanosis because they cannot breathe through the nose at all.
• When this malformation is confined to the posterior nostril on one side of the nasal passages, you may breathe almost normally or you may experience severe shortness of breath.
• Severe dyspnea is common with systemic cyanosis.
• When trying to breathe, the chest cavity may be sucked into the chest cavity.
• It is common for cyanosis to go away temporarily or to lessen because babies can open their mouths and breathe through their mouths while they cry.
• It is a malformation that cannot properly suck milk or artificial nutrition and is very dangerous for basic life support.
Diagnosis of Choanal atresia
• A feeding tube or a probe that goes into the nasal cavity through the nostril is inserted to check whether the tube passes through the nostril and into the nasal cavity and then passes through the posterior nostril into the pharyngeal cavity. is also diagnosed (see Figures 101 and 102).
• Diagnosis can be made by inserting a contrast object through the nostril into the nasal cavity and taking an X-ray of the nose to see if the contrast material is leaking into the upper pharyngeal cavity.
• Diagnosis can be made with a probe as shown in Figures 101 and 102.
• When you block your nostrils with a bulb syringe, you can diagnose by knowing whether the inside of the bulb syringe is filled with the air you breathe.
• Diagnosis can be made by nasal CT scan.
Treatment of Choanal atresia
• Get emergency treatment.
• Breathe through the mouth.
• First, an oral airway tube is placed in the mouth and allowed to breathe through it, and the obstructed posterior nostril is surgically treated as early as possible.
• An oral airway tube is inserted into the mouth to breathe through the airway tube, and timely, selective surgical treatment is performed.
• Surgery is performed through the nostril and results are generally good.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy of Pediatrics
-
drleepediatrics.com제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gerhon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”