신생아 무항문(쇄항문/쇄항증/무항증/무 항문증) Imperforate anus of newborn infants

그림 54. 여러 종류의 쇄항증.
화살 표시로 가르킨 부분의 직장이아 항문 부분이 막혀 있다.
Used with permission from Ross lab Columbus Ohio와 소아가정간호백과
- 태어날 때부터 항문의 일부분이나 전부가 불완전하게 또는 완전히 막혀 있는 선천성 기형을 쇄항증, 무항증, 무 항문증, 또는 항문 막힘이라 한다.
- 항문이 완전히 막힌 쇄항증도 있고, 불완전하게 막혀서 항문에 작은 항문 구멍이 조금 뚫려 있는 쇄항증도 있다.
- 항문만 막힌 쇄항증도 있고 항문의 바로 위에 있는 직장이 완전히 막힌 쇄항증도 있다.
- 항문의 전부가 완전히 막혔을 때는 막힌 항문의 부분의 바로 위에 있는 직장관 속에서 방광 속이나 직장관 속 주위에 있는 다른 기관 속과 연결되는 누관(루(漏)/누출관/Fistula)이 선천성으로 생길 수 있다.
- 다시 설명하면, 막힌 항문 바로 위에 있는 직장관 속과 방광 속이나, 질강 속, 또는 요도관 속에 연결되어 있는 누관(루)이 생길 수 있다.
- 대변이 항문을 통해 정상적으로 나오는 대신 대변이 이런 누관(루) 속을 통해 질강 속, 방광 속, 요도관 속, 또는 외음부 등으로 흘러나올 수 있다.
- 쇄항증이 있는 아이에게 선천성 척수신경 기형, 또는 선천성 비뇨기 기형이 함께 생길 때도 있다.
신생아의 무항문의 증상 징후

사진 55. 쇄항증이 있는 여 영아의 항문 주위.
선천적으로 항문이 막혀 항문이 없다.
CopyrightⒸ 2011 John Sangwon Lee,MD., FAAP
- 쇄항증의 정도와 그 주위에 생긴 선천성 기형의 유무 등에 따라 증상 징후가 다르다.
- 항문이 완전히 막히지 않고 항문에 작은 구멍이 뚫린 쇄항증이 있을 때는 출생 후 태변이 국수가닥처럼 가늘게 조금씩 나올 수 있다.
- 완전히 막힌 쇄항증이 있을 때는 태변을 전혀 볼 수 없다.
- 항문이 완전히 막혔을 때는 출생 후 항문에서 태변이 조금도 나올 수 없고 위장의 가스가 항문을 통해서 조금도 배출되지 않기 때문에 배가 부르고 구토할 수 있다.
- 막힌 항문 부위 바로 위 직장관 속과 방광 속이나 질강 속을 연결하는 누관(루)이 있을 때는 태변, 대변 및, 또는 가스가 그 누관(루)을 통과해 방광 속이나 질강 속 등으로 나올 수 있다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제3권 신생아, 영유아, 학령기와 사춘기 아이들의 성장발육-신생아 항문 참조.
신생아의 무항문의 진단 치료
- 병력, 증상 징후 진찰소견 등을 종합하여 진단한다.
- 육안으로 쉽게 볼 수 있는 쇄항증은 항문검진으로 진단할 수 있다.
- 항문 바깥에서 안쪽으로 좀 멀리 떨어진 항문 부분에 생겨 있는 쇄항증은 육안으로 쉽게 볼 수 없다.
- 체온을 재기 위해 항문 체온계를 갓 태어난 신생아의 항문 속에 넣을 때 항문이 막혀 있는 것을 처음으로 발견되어 쇄항증을 진단하기도 한다.
- 태어난 후 1∼2일이 지난 후에도 태변을 전혀 보지 않거나 태변이 국수가닥처럼 가늘게 조금씩 나오거나 쇄항증의 증상 징후가 있으면 쇄항증을 의심 한다.
- 복부 X선 사진검사, 복부 초음파 사진 검사 등으로 진단할 수 있고 진단 결과에 따라 수술로 치료한다.
- 무항문증을 아래 그림 56~59에서 볼 수 있는 것 같이 Ⅰ, Ⅱ, Ⅲ, Ⅳ형으로 나눈다.
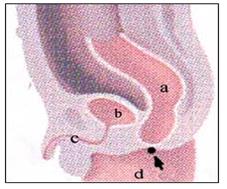
그림 56. 무 항문증(쇄항증) Ⅰ형
a-직장, b-방광, c-요도, d-항문이 있어야 할 부분에 항문이 없다.
출처; Used with permission from Ross Lab, Columbus. Ohio. USA와 소아가정간호백과
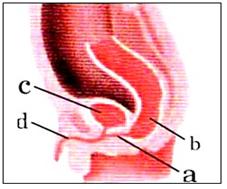
그림 57. 무 항문증(쇄항증) Ⅱ형
a-직장-요도 간 누관(루), b-무 항문과 직장, c-방광, d-요도.
출처; Used with permission from Ross Lab, Columbus. Ohio. USA와 소아가정간호백과
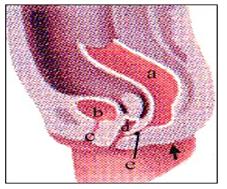
그림 58. 무 항문증(쇄항증) Ⅲ형
a-직장, b-방광, c-요도, d-질강 e- 직장과 질강 속 간 루, 화살로 표시된 부위는 항문이 있어야할 부위에 항문이 없다.
출처; Used with permission from Ross Lab, Columbus. Ohio. US와 소아가정간호 백과
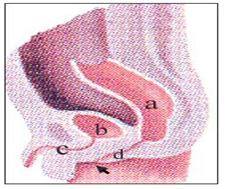
그림 59. 무 항문증(쇄항증) Ⅳ형
a-직장, b-방광, c-요도, d-직장의 하단 부분이 비정상적으로 좁아졌다. 화살로 표시된 부위가 거의 막힌 항문 부위다. 출처; Used with permission from Ross Lab, Columbus. Ohio. USA와 소아가정간호백과
Imperforate anus of newborn infants 신생아 무항문(쇄항문/쇄항증/무항증/무 항문증)
Fig. 54. Different types of sequelae. The rectum at the point pointed by the arrow mark, and the anus part is blocked. Used with permission from Ross lab Columbus Ohio and Pediatric Home Nursing Encyclopedia
• Congenital anomalies in which part or all of the anus is incompletely or completely blocked from birth is called astaxia, asthenia, anorectosis, or anal blockage.
• In some cases, the anus is completely blocked, and in some cases, the anus is incompletely blocked and a small anal hole is opened in the anus.
• Some with only anus obstruction, and some with complete obstruction of the rectum directly above the anus.
• When the entire anus is completely blocked, a fistula (ru/leak tube/Fistula) that connects to the inside of the bladder or other organs around the rectal canal is congenital in the rectal canal just above the blocked anus. Can occur.
• In other words, a fistula (fistula) that is connected to the rectal and bladder, vaginal cavity, or urethra that is just above the blocked anus may occur.
• Instead of stool coming out normally through the anus, stool may flow into the vaginal cavity, bladder, urethra, or vulva through these fistulas.
• In some cases, congenital spinal nerve anomalies or congenital urinary anomalies may be present in children with seizures. Signs of symptoms of anus in newborns
Picture 55. Around the anus of a girl infant with atresia. There is no anus due to congenital blockage of the anus. CopyrightⒸ 2011 John Sangwon Lee, MD., FAAP
• Symptoms and signs differ depending on the degree of seizure and the presence or absence of congenital anomalies around it.
• If the anus is not completely blocked and there is a small hole in the anus, the meconium may come out little by little after birth.
• You cannot see meconium at all when you have a completely blocked catechesis.
• When the anus is completely blocked, no meconium can come out of the anus after birth, and no gas in the stomach is discharged through the anus, so the stomach may become bloated and vomiting.
• When there is a fistula (fistula) that connects the rectal duct directly above the blocked anal area into the bladder or vaginal cavity, the meconium, feces, or gas may pass through the fistula (loo) and exit into the bladder or vaginal cavity. have. [Parents should also be anti-doctors-Pediatric Family Nursing Encyclopedia]-Volume 3 Growth and Development of Newborns, Infants, School-Age and Adolescent Children-Newborn See Anal.
Diagnosis, treatment of anus in newborns
• Comprehensive diagnosis including medical history, symptoms, symptoms, and examination findings.
• Stroke, which can be easily seen with the naked eye, can be diagnosed with an anal examination.
• Stroke in the anus that is a little farther inward from the outside of the anus is not easily visible with the naked eye.
• When an anal thermometer is inserted into the anus of a newborn baby to measure the body temperature, it is the first time that the anus is found to be blocked, and it is sometimes diagnosed with seizure.
• One to two days after birth, if you do not see meconium at all, or if the meconium comes out little by little like noodles, or if there are symptoms of seizure, you suspect seizure.
• It can be diagnosed with an abdominal x-ray photo test, an abdominal ultrasound photo test, etc., and treated with surgery according to the diagnosis result.
• As shown in Figures 56~59 below, an analosis is divided into types Ⅰ, Ⅱ, Ⅲ, and Ⅳ.
Figure 56. Anorectomy (Chestochrome) Type Ⅰ There is no anus in the area where the a-rectum, b-bladder, c-urethra, d-anus should be. source; Used with permission from Ross Lab, Columbus. Ohio. USA and Pediatric Home Nursing Encyclopedia
Figure 57. Anorectomy (Chestochrome) Type Ⅱ a-rectal-urethral fistula (fistula), b-no anus and rectum, c-bladder, d-urethra. source; Used with permission from Ross Lab, Columbus. Ohio. USA and Pediatric Home Nursing Encyclopedia
Figure 58. Anorectomy (Chestochrome) Type Ⅲ a-rectum, b-bladder, c-urethra, d-vaginal cavity e- rectal and intravaginal fistula, the area marked with an arrow does not have an anus in the area where the anus should be. source; Used with permission from Ross Lab, Columbus. Ohio. US and Child and Family Nursing Encyclopedia
Figure 59. Anorectomy (Chestochrome) Type IV The lower part of the a-rectum, b-bladder, c-urethra, and d-rectum was abnormally narrowed. The area marked by an arrow is the area of the anus that is almost blocked. source; Used with permission from Ross Lab, Columbus. Ohio. USA and Pediatric Home Nursing Encyclopedia
출처 및 참조문헌
- www.drleepediatrics.com제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”