수정체 후 섬유증식증과 미숙 신생아 망막증(미숙아 망막병증) Retrolental fibroplasia (Retinopathy of prematurity/ROP)
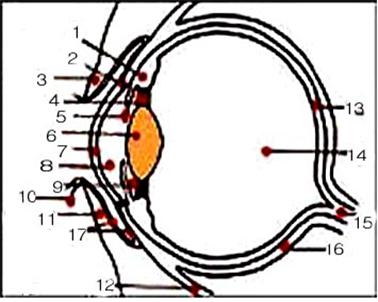
그림 115.
1-모양체(섬모층),
2-쉴렘관,
3-위 눈꺼풀,
4-렌즈 소대(지지인대),
5-홍채,
6-수정체(렌즈),
7-각막,
8-전방,
9-후방,
10-눈썹,
11-아래 눈꺼풀,
12-안구하직근,
13-망막,
14-초자체,
15-시신경,
16-공막,
17-아래 결막
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
-
망막은 안구의 후방에 있으면 전체 안구의 후방의 맨 뒤 표면의 3/4정도를 차지하고 있다.
-
그 망막에 퍼져 있는 모세혈관에 병변이 생기고 렌즈의 뒷부분에 섬유증식증이 생겨 시력이 감소되거나 시력이 아주 상실될 수 있는 눈병을 수정체 후 섬유증식증이라고 정의 했었다.
-
그러나 요즘에는 수정체 후 섬유증식증이란 병명 대신 미숙아 망막증, 또는 미숙아 망막병증
-
(Retinopathy of prematurity/ROP)이라는 병명을 대신 쓴다.
수정체 후 섬유증식증과 미숙 신생아 망막증의 원인
-
아직도 원인은 확실히 모른다.
-
그러나 이 병은 미숙 신생아들의 망막의 혈관에 주로 생기는 망막 병으로 알려졌다.
-
특히 신생아 중환자실 집중치료를 받았던 미숙 신생아들에게 이 병이 생길 가능성이 더 많이 있다.
-
1940~1950년대, 미숙 신생아들에게 생긴 호흡곤란 증후군을 고농도 산소로 치료를 많이 했었다.
-
그런 고농도 산소 치료를 받은 미숙 신생아들에게 망막 병증이 생기고 그로 인해 그들의 일부는 시야를 잃었다.
-
그 후 1970~1980년에는 어떤 이유로든 미숙 신생아들에게 산소호흡 치료를 할 때는 산소의 혈중농도를 적절히 조절하면서 치료했다.
-
또 미숙 신생아의 질병과 건강을 전반적으로 보다 더 효과적으로 치료하고 관리함에 따라 미숙 신생아들에게 망막 병증이 훨씬 덜 발생했다. 그리고 그들에게 시력 상실이 생기는 확률이 아주 감소됐다.
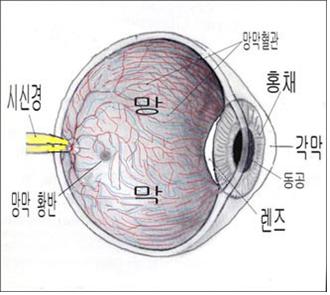
그림 116. 망막과 망막혈관
Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
-
요즘 미숙아에게 생기는 망막증은 고농도 산소치료로 인해 발생하는 비율보다 태어난 신생아가 미숙하면 미숙할수록 그 미숙 신생아에게 망막증이 생길 가능성이 더 많다.
-
과 산소 혈증, 수혈, 뇌실 내 출혈, 무호흡증, 감염, 비타민 E 결핍증, 출생 전 합병증 등의 질병이나 증상이 미숙 신생아에게 있을 때 미숙아 망막증이 생길 확률이 더 많다고 한다.
-
미숙 신생아의 혈중 산소농도가 비정상으로 더 높을 때 이 병이 생길 수 있고 미숙아 특발성 호흡곤란증후군 (“부모도 반의사가 되어야한다–소아가정간호백과“제6권 신생아 성장 발육 양호 및 질환 –특발성 호흡곤란증후군 참조)을 고농도 산소로 치료할 때 혈중 산소농도가 비정상적으로 높으면 이 병이 생길 수 있다.
-
이 병은 아직 출생되지 않은 태아에게도 생길 수 있고 고농도 산소 호흡치료를 받지 않은 미숙 신생아에게도 생길 수 있고, 또 만삭에 태어난 신생아에게도 생길 수 있다.
-
고농도 산소호흡 치료 이 외 다른 원인으로도 이 병이 생길 수 있다.
수정체 후 섬유증식증과 미숙 신생아 망막증의 증상 징후
-
미숙아 망막 병증이 처음 시작할 때는 안과 전문의가 진찰을 하지 않고 일반 비 의료인이 그냥 눈을 보고서 눈에 어떤 이상이 있는 지 분간하기가 곤란 하다.
-
화아에게 아무 증상이나 징후가 나타나지 않는 것이 보통이다.
-
그렇지만 이 병의 초기에 안과에서 자세히 검사하면 눈의 망막에 이 병으로 병변이 시작되고 있는 것을 알아 낼 수 있다.
-
망막에 생긴 병변의 진행 정도에 따라 안과에서는 미숙아 망막증을 5단계로 구분한다.
-
이 병이 시작될 때 망막의 모세혈관이 막힐 수도 있다.
-
이런 병변이 생기기 시작한 후 첫 6개월 동안 병변이 점점 계속 악화될 수 있고 망막 이탈증 또는 녹내장 등이 동시 생길 수 있다.
-
심하면 망막 조직이 섬유질 조직으로 대체되기도 하고 시력이 완전히 상실될 수 있고 일부 상실될 수 있다.
-
미숙아 망막증은 갑자기 생기지 않고 서서히 생기는 것이 보통이다.
-
이 병이 계속 진행되고 병변이 극도로 악화될 때에는 시력이 완전히 상실되고 맹인이 될 수 있다.
-
이 병이 서서히 진행되다가 더 이상 진행되지 않을 수도 있다.
-
이 때는 근시나 사시 또는 소안(小眼) 등이 생길 수 있다.
수정체 후 섬유증식증과 미숙아망막증의 진단
-
병력·증상 징후와 안과 진찰소견을 종합해서 이 병을 진단할 수 있다.
-
특히 미숙 신생아에게 고농도 산소호흡 치료를 했을 때는 이 병이 발생될 가능성이 더 있다.
-
미숙 신생아들에게 이 병의 증상 징후가 나타나기 전에 의사의 지시에 따라 미숙 신생아들은 이런 병이 생기는지 눈 검사를 주기적으로 받아야 한다.
-
일반적으로 미숙 신생아들이나 특히 신생아 중환자실에서 산소호흡 치료를 받았던 미숙 신생아들은 생후 몇 개월 동안 주기적으로 안과에서 눈을 검사받고 이런 병이 생기는지 조기에 진단해서 적절한 치료를 받아야 한다.
수정체 후 섬유증식증과 미숙 신생아 망막증의 치료
-
만삭 신생아들이나 미숙 신생아들이 고농도 산소 치료를 받았을 때 그들에게도 이 병이 발생될 가능성이 있다.
-
특히 체중이 아주 적게 태어난 미숙 신생아들이 고 농도 산소호흡 치료를 받았을 때는 이 병이 생길 가능성이 있기 때문에 극히 주의해서 산소호흡 치료를 해야 한다.
-
미숙 신생아에게 산소호흡 치료를 할 때 이 병이 발생될 가능성이 있지만 산소호흡 치료를 꼭 해야 할 때는 이 병이 발생될 위험성이 있더라도 산소호흡 치료를 할 때가 많다.
-
혈 중 산소 농도가 비정상적으로 높으면 높을수록 이 병이 발생될 가능성이 더 많다.
-
그러나 산소호흡 치료로 인해 이 병이 생기는 가능성보다 미숙 신생아가 더 미숙할수록 이 병이 생길 가능성이 더 많다.
-
신생아에게, 특히 미숙 신생아에게 산소호흡 치료를 할 때 혈중 산소 농도를 자주 측정하면서 산소호흡치료를 해야 한다.
-
이 병이 일단 시작해서 계속 진행할 때는 특별한 치료 방법이 아직 없지만 요즘은 조기 주변 망막 박리치료를 조기에 해서 치료한다.
-
미숙신생아가 산소 호흡치료를 받을 때 비타민 E를 섭취하면 이 병이 예방될 수 있다고 하나 그 약 치료효과는 아직 확실치 않다.
-
이 병으로 시력 이상이 생긴 아이들은 안과 전문의의 진단 치료를 주기적으로 계속 받을 필요가 있다.
-
이런 치료는 어디까지 의사의 지시에 따라 할 일이지만 미숙 신생아를 양육하는 부모들도 이런 병에 대해서 참고로 알아둘 필요가 있다.
Retrolental fibroplasia (Retinopathy of prematurity/ROP)
Figure 115. 1 – ciliary body (ciliary layer), 2 – Schlemm’s Hall, 3 – upper eyelid, 4-lens platoon (support ligament), 5 – iris, 6 – lens (lens), 7 – cornea, 8 – anterior, 9 – rear, 10 – eyebrows, 11 – lower eyelid, 12 – rectus subocular muscle, 13 – retina, 14 – vitreous, 15 – optic nerve, 16 – sclera, 17 – lower conjunctiva Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
• When the retina is in the back of the eyeball, it occupies about 3/4 of the rearmost surface of the entire eyeball.
• Post-lens fibrosis was defined as an eye disease in which a lesion occurs in the capillaries spread in the retina and fibrosis occurs in the back of the lens, leading to reduced or even loss of vision.
• However, nowadays, instead of the disease called post-lens fibrosis, retinopathy of prematurity, or retinopathy of prematurity
• Use the disease name (Retinopathy of prematurity/ROP) instead.
Causes of post-lens fibrosis and retinopathy of prematurity
• The cause is still unknown.
• However, this disease is known to be a retinal disease that mainly occurs in the retinal blood vessels of premature newborns.
• Premature newborns who have received intensive care in neonatal intensive care units are more likely to develop the disease.
• In the 1940s and 1950s, respiratory distress syndrome in premature newborns was often treated with high-concentration oxygen.
• Premature newborns who received such high-oxygen therapy developed retinopathy, which resulted in some loss of vision.
• From 1970 to 1980, when oxygen respiration therapy was administered to premature newborns for any reason, the oxygen concentration was appropriately controlled.
• In addition, preterm newborns are far less likely to develop retinopathy as their disease and health are more effectively treated and managed overall. And their chances of losing sight are greatly reduced.
Figure 116. Retina and retinal vessels Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
• Retinopathy occurring in premature infants these days is more likely to develop in premature newborns than the rate that occurs due to high-concentration oxygen therapy.
• Premature infants are more likely to develop retinopathy of prematurity when they have diseases or conditions such as hyperoxemia, blood transfusions, intraventricular hemorrhage, apnea, infection, vitamin E deficiency, and prenatal complications.
• This disease can occur when the blood oxygen concentration of premature newborns is abnormally high, and idiopathic respiratory distress syndrome (Idiopathic Respiratory Distress Syndrome in premature babies) This disease may occur if the oxygen concentration in the blood is abnormally high when high-concentration oxygen is used for treatment of difficult syndrome).
• The disease can occur in unborn fetuses, in premature newborns who have not received high-oxygen breathing therapy, and in newborns born in full term.
• Causes other than high oxygen breathing therapy can also cause this disease.
Symptoms, signs of post-lens fibrosis and retinopathy of prematurity
• When retinopathy of prematurity first begins, it is difficult for non-medical personnel to see what is wrong with the eyes without an ophthalmologist examining them.
• It is normal for Hwa-ah to show no symptoms or signs.
• However, detailed examination by an ophthalmologist in the early stages of the disease can reveal the onset of the disease in the retina of the eye.
• According to the degree of progression of the retinal lesion, ophthalmology classifies retinopathy of prematurity into 5 stages.
• Capillaries in the retina may become blocked when the disease begins.
• During the first 6 months after these lesions begin to develop, the lesions may continue to worsen, and retinal detachment or glaucoma may occur simultaneously.
• In severe cases, retinal tissue may be replaced by fibrous tissue, and vision may be completely or partially lost.
• Retinopathy of prematurity does not occur suddenly but usually develops slowly.
• As the disease progresses and the lesion becomes extremely severe, complete loss of vision and blindness may occur.
• The disease progresses slowly and may not progress any further.
• At this time, myopia, strabismus, or small eyes may occur.
Diagnosis of post-lens fibrosis and retinopathy of prematurity
• This disease can be diagnosed by combining the medical history/symptoms, signs, and ophthalmological examination findings.
• This disease is more likely to develop, especially when high-concentration oxygen-breathing therapy is given to premature newborns.
• Before premature newborns show symptoms of the disease, as directed by a doctor, premature newborns should have their eyes checked regularly for these conditions.
• In general, premature newborns, especially premature newborns who have received oxygen-breathing therapy in the neonatal intensive care unit, should have their eyes checked by an ophthalmologist periodically during the first few months of life, and early diagnosis of these diseases should be provided for appropriate treatment.
Treatment of post-lens fibrosis and retinopathy of prematurity
• When full-term or premature newborns receive high-oxygen therapy, there is a possibility that they will also develop the disease.
• Oxybreathing treatment should be performed with extreme caution, especially since premature newborns born with very low birth weight are more likely to develop this disease when they receive high-concentration oxygen-breathing therapy.
• There is a possibility that this disease can occur when oxygen-breathing therapy is given to premature newborns, but when oxygen-breathing therapy is absolutely necessary, oxygen breathing therapy is often used even though there is a risk of developing this disease.
• Abnormally high levels of oxygen in the blood are more likely to develop the disease.
• However, premature newborns are more likely to develop the disease than it is due to oxygen-breathing therapy.
• When administering oxygen respiration therapy to newborns, especially premature newborns, oxygen respiration therapy should be performed while measuring blood oxygen levels frequently.
• When this disease starts and progresses, there is no specific treatment yet, but these days, early peripheral retinal detachment treatment is used to treat it.
• It is said that taking vitamin E when premature newborns receive oxygen breathing therapy can prevent this disease, but the therapeutic effect of the drug is still unclear.
• Children who have vision problems due to this disease need to continue to receive regular diagnostic treatment from an ophthalmologist.
• Such treatment should be done according to the doctor’s instructions, but parents of premature newborns need to be aware of these diseases as a reference.
출처 및 참조문헌
- www.drleepediatrics.com 제 6권 신생아 성장 발육 육아 질병
-
www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”