수막구균 뇌막염(수막구균 수막염)과 수막구균 패혈증, 피부 발진. Meningococcal meningitis and Meningococcal septicemia, skin rashes
(You may visit www.drleepediatrics.com – Chapter 7,
Pediatric Adolescent Infectious Diseases or제 7권, 소아 청소년 감염병 질환 웹사이트)
수막구균 뇌막염의 원인
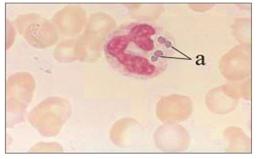
그림 2-64. 백혈구 내에 수막구균이 있는 것을 보고 진단할 수 있다.a-백혈구 속에 있는 수막구균. Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
-
수막구균(Neisseria meningitidis/ meningococcus)은 박테리아의 일종이고 수막염(구)균 또는 수막알구균이라고 한다.
-
수막구균(수막염구균) 감염으로 뇌막(수막)에 생긴 감염병을 수막구균 뇌막염, 또는 수막구균 수막염이라 한다.
-
수막구균 뇌막염은 일종의 세균성 뇌막염(박테리아 뇌막염)이다.
-
여기서 편의상 수막구균 뇌막염을 “뇌막염“이라고 칭한다.
-
수막구균이 핏 속으로 감염되면서 전신에 퍼져 전신 수막구균 염증을 일으키는 감염병을 수막구균 패혈증이라고 한다.
표 2-4.수막구균에 수막(뇌막)이 감염되면 다음과 같은 수막구균 감염병이 발생될 수 있다.
| 전염병의 종류 | 발생% |
| 뇌수막염 | 47% |
| 뇌막 구균성 패혈증 | 43% |
| 폐렴 | 6% |
| 그 외 | 3.4% |
출처; Rosenstein NE, et al. J Infect Dis. 1999; 180:1894-1901
-
급성 전격성 수막구균 패혈증· 후두개염· 중이염· 결막염· 화농성 관절염· 화농성 심낭염· 만성 수막구균 패혈증 등 수막구균 감염병이 발생될 수 있다.
-
건강한 아이들이나 성인들의 인두 점막층, 비강 점막 층에 수막구균을 평소에 보균하고 있을 수 있지만, 수막구균 뇌막염이나 수막구균 패혈증이 잘 생기지 않는 것이 보통이다.
-
어떤 사람에게는 수막구균 뇌막염이나 수막구균 패혈증이 생길 수 있고, 또 다른 사람에게는 수막구균 뇌막염이나 수막구균 패혈증이 생기지 않는 이유는 확실히 모른다.
-
이 병을 앓는 사람이 호흡할 때, 또는 말 할 때 수막구균이 든 침이나 가래, 비말(飛沫) 등을 통해 다른 사람들에게 수막구균이 감염될 수 있다.
-
연령에 관계없이 모든 사람들에게 이 병이 생길 수 있다. 그러나 생후 6∼12개월 영아들에게 이 병이 더 잘 발생될 수 있다.
-
아무 병을 앓지 않는 건강한 아이들에게도 이 병만 발생할 수 있지만 감기나 다른 종류의 바이러스성 상기도 염을 앓는 아이들에게 이 병이 더 잘 발생될 수 있다.
-
상기도 염을 2∼4일 동안 앓다가 수막구균에 감염되어 수막구균 뇌막염 및, 또는 수막구균 패혈증이 생길 수 있다.
-
이 병은 군 장병들이나 학교, 또는 탁아소 등 집단생활을 하는 성인들이나 소아청소년들에게 더 잘 발생할 수 있다.
-
잠복기는 1∼10일이다.
수막구균 뇌막염의 증상 징후
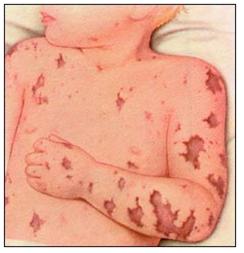
그림 2-65. 수막구균 뇌막염으로 전신 출혈 반점이 생길 수 있다. 출처;Used with permission from Ross Labotories,Columbus, Ohio,USA
-
수막구균 뇌막염의 증상 징후는 다양하다.
-
때에 따라 증상 징후는 많이 다르다.
-
전형적인 증상 징후는 다음과 같다.
-
수막구균이 체내에 감염된 후 감기와 비슷하게 1∼2일 동안 앓다가 갑자기 고열과 두통 등 생명에 위중한 독성 상태의 증상 징후가 생기면서 몹시 아픈 것 같이 보인다.
-
바로 독성 상태에 빠지게 된다. 아주 드물게는 며칠 동안 신음하면서 경미하게 앓을 수 있다.
-
수막구균 뇌막염이 발생되면 갑자기 고열이 나면서 생명을 위협할 정도 위중하게 앓는 것이 보통이다.
-
수막구균이 체내에 감염된 후 불과 몇 시간 내 급속도로 전신으로 퍼져 수막구균 패혈증 및, 또는 뇌막염이 생길 수 있다.
-
수막구균 패혈증 및, 또는 뇌막염이 생기면 몹시 탈진되고 온몸의 힘이 쭉 빠지고, 몸이 축 늘어지고, 비정상적으로 잠만 자고, 전신경련을 할 수 있다.
-
심한 두통·오한·구토·전신 권태·관절통 등의 증상 징후가 계속 될 수 있고 여러 가지 크기의 출혈반점이 피부와 점막에 나타날 수 있다(그림 2-65 참조).
-
[부모도 반의사가 되어야 한다–소아가정간호백과]-제17권 소아청소년 피부질환–머리, 얼굴 등에 생긴 점상출혈, 피부 발진(열꽃)과 열이 나는 질병들 중 수막구균 패혈증 참조.
-
때로는 전신 피부에 출혈이 생겨 신체의 전 피부와 점막에 피가 맺히고 출혈반점이 생길 수 있다.
-
이 병은 조기에 진단해서 적극적으로 치료하지 않으면 짧은 시간 내 사망하는 것이 보통이다.
수막구균 뇌막염의 진단
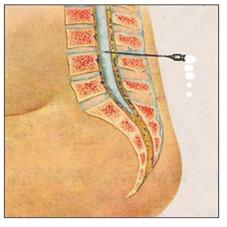
그림2-66.뇌염이나 수막염(뇌막염)이 의심되면 요추 천자로 뇌척수액을 뽑아 검사한다.
Copyright ⓒ 2013 John Sangwon Lee, M.D. FAAP
-
병력·증상 징후·진찰소견 등을 종합하여 이 병이 의심되면 피, 뇌척수액, 소변, 피부 발진 등에서 피검물을 채취해서 그것으로 그람 염색 현미경 수막구균 세균검사 및 세균 배양 검사 등을 한다.
-
소변, 피, 뇌척수액 등으로 수막구균 항원 항체 응집 반응 검사를 해 진단할 수 있다.
-
일반적으로, 이 병으로 생긴 증상 징후와 진찰소견을 종합해서 이 병을 진단할 수 있을 때는 생명이 위험할 정도로 이미 병이 많이 진행된 상태일 때가 많다.
수막구균 뇌막염의 치료
-
이 병은 정말로 응급 중 응급으로 치료해야 한다.
-
이 병에 걸렸다고 의심하면 속히 치료하기 위해 병원 입원수속을 하기도 전 원인이 될 수 있는 세균 검사를 하는 데 필요한 피, 뇌척수액, 또는 다른 적절한 피검 물을 가능한 한 응급으로 속히 채취해야 한다.
-
그와 동시, 페니실린이나 다른 적절한 항생제 혈관주사 치료를 즉시 하기 시작해야 한다.
-
또한 포도당 전해질용액 혈관주사 치료를 시작하고, 그때그때 생긴 증상 징후에 따라 대증 치료를 한다.
-
환아가 페니실린에 알레르기가 있으면 클로램페니콜(Chloramphenicol), 세포택심(Cefotaxime), 또는 그 외 다른 적절한 항생제 혈관주사로 응급 치료를 시작한다.
-
때와 장소에 따라 세균검사를 할 수 있는 피검 물을 채취하기도 전 항생제를 정맥혈관주사로 주어 응급 치료를 해야 할 때도 있다.
무균성 뇌막염(무균성 수막염/Aseptic meningitis)과 박테리아 뇌막염(Bacterial meningitis)를 감별진단 하는데 프로칼시토닌(Procalcitonin) 검사를 이용한다.
환자와 접촉한 경우
-
수막구균 뇌막염 및, 또는 수막구균 패혈증을 앓는 환아와 근접하거나 접촉한 성인들이나 소아청소년들, 또는 그의 가족들, 의사나 간호사가 이 병에 걸리지 않도록 경구용 리팜핀(Rifampin) 등 항생제로 예방적 항생제 치료를 받아야 한다.
-
이 병을 적절한 항생제로 적절히 치료 시작한 24시간 이후 환아를 더 이상 격리할 필요가 없다.
수막구균 감염으로 인한 감염병의 예방접종 Meningococcal Infection Immunization
-
다음 미 소아청소년 학회 권장 소아청소년 감염병 예방접종 스케줄 참조.
-
수막구균에 뇌막이 감염되어 수막구균 뇌막염을 일으킬 수 있고 그 수막구균이 전신의 혈액에 감염하여 수막구균 패혈증을 일으킬 수 있다.
-
때로는 수막구균 뇌막염과 수막구균 패혈증을 동시 생길 수 있다.
-
수막구균에는 13종의 혈청군이 있다. 대부분의 수막구균의 침입성 감염은 A군, B군, C군, Y군, W-135군 등에 의해 생긴다.
-
A군, C군, Y군, W-135군 혈청군의 수막구균에 의한 감염을 예방할 수 있는 수막구균 예방접종 백신이 있다. 수막구균 예방접종 백신에는 MPSV4 백신과 MCV4 백신이 있다. 그러나 B혈청군의 수막구균 감염을 예방을 할 수 있는 MenB-4C, Bexsero, MenB-FHbp, Trumenba 백신이 있다.
-
MPSV4 백신은 피하 주사로 접종할 수 있고 해부학적 무 비장 또는 기능적 무 비장이 있는 2~10세 된 아이들, 또는 말기 보체결핍증이 있는 아이들에게 예방접종할 수 있다.
-
MCV4 백신은 근육 주사로 접종할 수 있고 11~55세 연령층에 속한 사람들에게 예방접종할 수 있다. 그러나 MCV4 백신은 2~10세 아이들 중 고 위험군에 속한 건강 문제가 있는 아이들에게도 접종할 수 있다.
-
수막구균 감염으로 인한 감염병은 소아청소년들이나 성인들에게 발생될 수 있고 군대나 학교 또는 탁아소 등 집단생활을 하는 소아청소년들이나 성인들에게 더 잘 발생될 수 있다. 최근에는 10~12세 이상 사춘기 아이들에게 접종 해줄 수 있는 기본적 예방접종에 포함시킬 것을 권장한다.
-
침입성 수막구균 감염이 년 2200~3000명의 미국 사람들에게 발생되었고 십만 명의 영아들 중 0.9~1.5명, 2~4세 유아들 중 1.8명, 학령기 전, 학령기 아이들과 사춘기 아이들의 연령층에 있는 5~17세 아이들 중 0.7명, 18~34세 청장년들 중 0.7명에게 발생됐다는 연구도 있다.
-
침입성 수막구균 감염으로 심하게 앓다가 회복되거나 사망한 자녀들을 둔 부모들이 이 병을 예방할 수 있는 백신이 있는지 알지도 못하고 있었다는 예가 종종 있었다. 그러므로 이런 예방접종 백신이 있다는 사실을 부모들에게 알려 주어야 한다고 한다(표1과 표2 참조).
수막구균 백신
-
수막구균의 A, C, Y와 W-135 혈청군에 속하는 수막구균 감염으로 생긴 감염병을 예방할 수 있는 수막구균 백신에는 다음과 같은들이 있다. 즉Meningococcal¹³ (MenACWY-D 생후 9 개월이나 그후. MenACWY-CRM-D는 생후 2개월이나 그 이후. MenACWY-TT는 은 생후 2세나 그 이후. –
Meningococcal B 백신에는 MenB-4C, Bexsero, MenB-FHbp, Trumenba 백신이 있다. 10세나 그 이상에 접조한다. Bexsero백신은 2회 접종하고 Trumenba 백신은 총 3회 접종한다. 위험도다 없는 사춘기아이들이나 청년들은 16-23세에 접종받는다. 소스: CDC, AAP News 3/2021
접종 방법
-
건강검진을 받고 열이 있나 체온을 재고, 발열성 감염병이 없고 MCV4 백신이나 MPSV4 백신에 알레르기가 없고 그 접종을 받는데 금기 조건이 없으면 1차 접종을 받는다.
접종 효과
-
1차 접종을 받은 후 10~14일경에 예방될 수 있는 면역체가 나타난다.
-
연구에 의하면 2~4세 아이들이 A군 수막구균 예방접종을 받은 후 3년이 될 때 면역 효과는 67% 정도이다.
다음과 같은 경우 수막구균 감염병 백신으로 특별히 접종 받는다.
-
미국 CDC는 수막구균 감염을 예방하기 위해 건강한 소아청소년들이 11-12세에 1차, 16세에 2차 총 2회, 통상예방접종해 주라고 권장하고 있다.
-
비장이 없거나 비장 기능이 비정상적인 소아들, 면역체 결핍증이 있는 소아청소년들이나 선천성으로나 후천성으로 콤플리멘트(보체) 결핍증이 있는 소아들은 특별한 예방 접종스케줄에 따라 에방 접종을 받아야 환다.
-
수막구균 감염병이 많이 유행하는 지방이나 나라에 여행가는 사람들에게
-
살고 있는 지역에 이 병이 발생됐을 때
-
신병들과 대학생들, 특히 기숙사 생활하는 대학 신입생들에게
-
병원 임상 검사실에서 일하는 사람들에게
-
예방접종을 해주기를 요구하는 부모들의 소아청소년들에게는 특별한 스켜줄에 따라 접종한다.
-
그 외
접종 연령
-
예방 접종표 참조.
-
모든 건강한 소아청소년들에게 수막구균 감염병을 예방접종을 해주라고 권장한다.
-
그렇지만 11~70세 연령층에 있는 모든 아이들이나 성인들은 누구든지 예방접종을 받을 수 있다.
-
특히 11~12세 이상 사춘기 아이들은 수막구균 예방접종을 기본적으로 받으라고 권장한다.
접종 금기
수막구균 백신에 알레르기가 있거나 발열성 감염병이 있는 소아청소년들이나 성인들과 임신부들은 접종을 받을 수 없다.
접종 부작용
-
백신 주사 맞은 국소에 통증, 발적, 부종 등이 생길 수 있다. 드물게 알레르기 반응이 생길 수 있다.
-
더 자세한 정보는 www.vaccineshoppe.com을 참조.
-
[부모도 반의사가 되어야 한다–소아가정간호백과]-제2권 소아청소년 질병 및 안전사고 예방. 2015년 1월 미 CDC, 미소아청소년과 학회에서 권장하는 소아청소년 예방접종 스케줄 참조.
2021년 1월 이후 권장 미 0~18세 소아청소년 기본 예방접종 Recommended immunization schedule for 0~18 year old Americal children in Jan 1st 2021
|
☞ 각 나라에 따라 권장 기본 예방접종 스케줄이 다를 수 있다. |
2021년 1월 이후 권장 미 0~18세 소아청소년 기본 예방접종 스케줄과 표 1A
Recommended immunization schedule for persons aged 0 through 18 years since January 2021
| 예방접종 백신 종류/ 예방해 주는 감염병 | 출생 후 바로 | 생후 1개월 |
생후 2개월 |
생후 4개월 |
생후 6개월 |
생후 9개궐 |
생후 12개월 |
생후 15개월 |
생후 18개월 |
생후 19~23개월 |
생후 2~3세 |
생후 4~6세 |
생후 7~10세 |
생후 11~12세 |
생후 13~15세 |
생후 16~18세 |
||||||
| Hepatitis B¹ (HepB) /b 형 간염 | ←1차 접종 | ←2차 접종→ | ←3차 접종→ | |||||||||||||||||||
| Rotavirus²(RV) RV-1(2회분 배열 접종); RV-5(3 회분 배열 접종)/ 로타바이러스 감염병 | ←1차 접종→ | ←2차 접종→ | 각주 2 | |||||||||||||||||||
| Diphtheria, Tetanus, acellular Pertussis³(DTaP;<7세)/파상풍, 디프테리아, 백일 해 | ←1차 접종→ | →2차 접종→ | ←3차 접종→ | ←4차 접종→ | ←5차 접종→ | |||||||||||||||||
| Tetanus, Diphtheria, acellular Pertussis⁴ (DTap;7세나 >7세 파상풍, 디프테리아, 백일 해 | (Tdap) | |||||||||||||||||||||
| Haemophilus influenzae type b⁵(HIb)/ 히브 감염병 | ←1차 접종→ | ←2차 접종→ | 각주 5 | ←3차 또는 4차 접종 → 각주 5 | ||||||||||||||||||
| Pneumococcal conjugate⁶a, c (PCV13)/폐렴연쇄상구균 감염병 | ←1차 접종→ | ←2차 접종→ | ←3차 접종→ | ←4차 접종→ | ||||||||||||||||||
| Pneumococcal polysaccharide⁶bc (PPSV23) /폐렴연쇄상구균 감염병 | ||||||||||||||||||||||
| Inactivated Poliovirus⁷(IPV)(<18 세)/소아마비 | ←1차 접종→ | ←2차 접종→ | ←3차 접종→ | ←4차 접종→ | ||||||||||||||||||
| 예방 접종 백신 종류/예방해 주는 감염병 | 출생 후 바로 | 생후 1개월 |
생후 2개월 |
생후 4개월 |
생후 6개월 |
생후 9개궐 |
생후 12개월 |
생후 15개월 |
생후 18개월 |
생후 19~23개월 |
생후 2~3세 |
생후 4~6세 |
생후 7~10세 |
생후 11~12세 |
생후 13~15세 |
생후 16~18세 |
||
| Influenza⁸(IIV; LAIV) 1부에게는 2회분,각주 8 /인플루엔자 | ←매해 마다 접종 받는다 (11V 만)→ | ←매해 마다 접종 받는다 (II V 또는 LAIV)→ | ||||||||||||||||
| Measles, Mumps, Rubella⁹(MMR)/ 홍역, 풍진, 유행성 이하선염 | ←1차 접종→ | ←2차 접종→ | ||||||||||||||||
| Varicella ¹⁰ (VAR) /수두 | ←1 차 접종→ | ←2차 접종→ | ||||||||||||||||
| Hepatitis A¹¹ (HepA)/A형 간염 | ←2 회분→ 주서 11 | |||||||||||||||||
| (Human papillomavirus¹² (HPV2; 여성에게만 (HPV4; 여성과 남성 에게)/사람유두종 바이러스 감염병 | ←3회 분 배열 접종→ | |||||||||||||||||
| Meningococcal¹³ (MenACWY-D 생후 9 개월이나 그후후. MenACWY-CRM-D는 생후 2개월이나 그 이후. MenACWY-TT는 은 생후 2세나 그 이후. /수막구균 뇌막염과 그 외 감염병
—————————- Meningococcal B 백신에는 MenB-4C, Bexsero, MenB-FHbp, Trumenba 백신이 있다. 10세나 그 이상에 접조한다. Bexsero백신은 2회 접종하고 Trumenba 백신은 총 3회 접종한다. 위험도다 없는 사춘기아이들이나 청년들은 16-23세에 접종받는다. 소스: CDC, AAP News 3/2021 |
←주서 13→ | ←1차 접종→ | 추가 접종 | |||||||||||||||
|
|
접종을 권장 하는 나이의 범위, | ||
|
|
건강상 고 위험 군 아이들에게 접종을 권장하는 나이 |
무균 뇌막염(무균 수막염)과 박테리아(성) 뇌막염의 감별진단 Differential diagnosis of aseptic meningitis and bacterial meningitis
-
뇌막에 바이러스 감염, 뇌막에 비 박테리아 병원체 감염, 또는 뇌막 중금속 중독 등으로 생긴 뇌막염을 무균 뇌막염이라고 한다.
-
박테리아 뇌막염은 박테리아 감염으로 생긴 뇌막염을 말한다.
-
감염증을 진단하는데 CBC 피 검사, 그 외 혈액검사, C-반응 단백질 혈중농도, 프로칼시토닌(Procalcitonin, PCT) 정량검사 등이 유용하게 사용되고 있다.
-
그 중 프로칼시토닌 정량검사가 가장 유용한 진단 가치가 있다고 한다.
-
프로칼시토닌은 칼시토닌(Calcitonin) 호르몬의 전구물질이고 갑상선의 C 세포에서 생성된다. 프로칼시토닌은 정상 건강한 사람의 피 속에 분비되어 있지 않는다.
-
심한 전신 감염병이 있을 때는 프로칼시토닌의 혈중 농도가 100ng이거나 그 이상 증가될 수 있다.
-
소아 뇌막염(수막염)의 5%는 박테리아 뇌막염이고 나머지는 무균 뇌막염이다.
-
소아 뇌막염이 생기면 피에서 프로칼시토닌 정량검사, C-반응 단백질, 백혈구 총수, 호중구수 검사 등을 하고 뇌척수액을 뽑아 검사하는 것이 보통이다.
-
뇌척수액에서 단백질 농도, 포도당 농도, 백혈구 수, 호중구수, 그람 염색 현미경 세균검사, 박테리아 항원 검사 등으로 무균 뇌막염에 걸렸는지 박테리아 뇌막염에 걸렸는지 감별 진단하는 것이 보통이다.
-
이상 설명한 여러 가지 검사결과 중 프로칼시토닌 정량검사의 결과치가 비정상적으로 증가되면 박테리아(성) 뇌막염에 걸려있다고 진단할 수 있다.
-
따라서 뇌막염에 걸렸을 때는 이 검사가 상당히 중요하다.
|
다음은 “뇌막염”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 뇌막염에 관해서
Q.
안녕하세요. 저희 아이가 뇌막염에 걸려 2주 동안 치료를 받다가 9월 14일날 퇴원했습니다.
그런데 9월 19일부터 열이 나서 병원에 갔더니 또 뇌막염이라고 하더군요.
일주일도 안 되어 그럴 수 있나요? 병원 말로는 퇴원당시 척수검사 할 때 염증세포가 3개뿐이었다고 하던데요. 모든 아이들이 그 정도는 가지고 있다고 말하더군요.
예방법이나 예방 주사는 어떤 것이 있나요.
A.
수미님
안녕하세요. 좋은 질문해 주셔서 감사합니다.
자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답을 드리는데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
뇌막염(수막염)은 뇌막 바이러스 감염, 뇌막 박테리아 감염, 그 외 뇌막 병원체 감염 등으로 인해서도 생길 수 있습니다. 드물게는 뇌막에 화학물질 독성이나 백혈병 악성 세포 침범으로 비병원체 감염으로 뇌막염이 생길 수 있습니다.
뇌막염이 원인이 무엇인가에 따라서 증상, 징후 진단, 치료 등이 다르고 예후도 많이 다릅니다. 어떤 세균이나 바이러스 등 감염에 의해서 뇌막염이 생겼나 알려주시면 더 확실한 답변을 드릴 수 있습니다.
불완전하게 치료되었던 뇌막염이 재발될 수도 있고 또 다른 세균 감염에 의해서 새 뇌막염이 다시 생길 수 있습니다.
드물게는 비강과 수막 사이에 비정상적으로 누관(Fistula)이 있다든지, 어떤 선천성 기형이 수막과 연결되어 그 연결된 통로를 통해서 세균이 수막(뇌막)에 감염되어 뇌막염이 재발 될 수도 있습니다. 이런 경우는 사실상 아주 드뭅니다.
백혈구 감소증이나 면역체 결핍증 등으로 세균감염에 저항력이 약하거나 없을 때 뇌막염 등이 재발 될 수 있습니다.
때로는 뇌막염이 완전히 치료되지 않은 상태에서 치료를 중지한 후 얼마 있다가 그 뇌막염이 재발 될 수 있습니다. 이런 것을 일부 치료 된 뇌막염(Partial treated meningitis)이라고 합니다.
뇌척수액 검사를 하고 뇌 CT 스캔 검사 등을 해서 뇌 농양 등이 있나 알아보는 것도 중요합니다.
아기의 단골 소아청소년과 의사로부터 계속 치료를 받으시고 의사와 상담하시기 바랍니다.
[부모도 반의사가 되어야 한다–소아가정간호백과]-제2권 소아청소년 질병 및 안전사고 예방–수막구균 예방접종,
뇌막염 등을 참조하시기 바랍니다.
소아청소년과에서 진찰 진단 치료를 받고 상담하시기 바랍니다.
질문이 더 있으시면 다시 연락 주세요. 감사합니다. 이상원 드림
|
다음은 “뇌막염 추가질문이요…”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 뇌막염 추가질문이요…
Q.
바쁘신 중에도 자상한 답변을 해주시니 감사드립니다.
좀 더 구체적으로 궁금한 사항이 있어 몇 자 적습니다.
뇌막염에 걸렸던 제 아들은 이제 4개월 입니다. 처음 병원에 입원당시 염증 세포 수치가 95개라고 하더군요. 약 12일 정도 치료 후 3개로 떨어졌고 2주째 퇴원을 했습니다.
그때 소견으로는 바이러스에 의한 뇌막염으로서 뇌 MRI 촬영 및 피, 소변검사도 했으나 별 이상이 없다고 했습니다. 그런데 제가 궁금한 것은 퇴원한지 1주일도 되지 않아 염증세포가 12개로 늘어났다는 것입니다(약 5일). 아무리 면역력이 약한 소아청소년라고 하더라도 뇌막염이 감기처럼 쉽게 걸리고 또 쉽게 재발하는 병인가요? 병원 측에서 치료를 소홀히 하거나 아직 완치가 안 된 아이를 퇴원 시키지는 않았는지 의심스러운 생각이듭니다. 병원의 과실을 따지자는 것이 아니라 똑같은 일로 제 아이가 두 번 고통 받는 일이 없도록 하자는 생각에 글을 적었습니다.
그럼 수고하십시오.
A.
수미님
안녕하세요. 또 좋은 질문해 주셔서 감사합니다.
자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등의 정보를 많이 알수록 답변을 드리는데 도움이 됩니다. 주신 정보를 토대로 해서 답변을 드리겠습니다.
이제 무슨 병을 앓았었는지 조금 더 알 수 있습니다. 정보를 더 주셔서 감사합니다.
첫 번째 질문하셨을 때는 바이러스성 뇌막염 및, 또는 바이러스성 뇌염, 박테리아 뇌막염 또는 다른 원인으로 인한 뇌막염에 걸렸는지 모르는 상태에서 답변을 드렸습니다.
지금 아기가 다른 종류의 박테리아 뇌막염에 걸렸는지 바이러스성 뇌막염 및, 또는 뇌염에 걸렸는지, 또는 전에 있던 뇌병이 재발됐는지 그 병의 자연 진행 경과 상태를 가지고 걱정하고 있는지 확실히 알 수 없습니다.
뇌척수액이나 뇌막이나 뇌에서 얻은 피검 물로 바이러스 배양이나 또는 박테리아 배양을 해서 뇌막염 및, 또는 뇌염의 원인이 되는 병원체가 무엇인지를 확실히 아는 방법도 있습니다. 일반적으로 뇌척수 액으로 바이러스 배양 검사를 많이 하지 않습니다.
뇌척수액 세균 배양검사에서 박테리아가 배양되지도 않으면 바이러스 감염으로 뇌막염이 생겼다고 역으로 진단하는 것이 통례입니다.
과거 한때 환자들이 자기들 마음대로 항생제를 약국에서 사서 자기들 맘대로 병을 치료했던 시절에는 박테리아 뇌막염을 앓고 있는 아이에게 감기를 앓는다고 부모들이 그들 마음대로 항생제 치료를 해서 그 항생제 치료로 인해서 박테리아 뇌막염이 일부만 치료되고 완치 되지 않고 박테리아 뇌막염이 만성적으로 진행되기도 했습니다. 그 만성 박테리아 뇌막염이 다시 급성 뇌막염으로 재발되기도 했습니다.
원인을 확실히 찾을 수 없이 고열이 날 때 뇌척수액 검사를 할 때가 소아청소년과에서는 흔합니다.
뇌척수액을 검사하기 전에 뇌막염 이외 다른 종류의 감염병이 있다고 진단하고 그 감염병을 항생제로 불완전하게 치료 받고 있는 중 박테리아 뇌막염을 앓는다고 의심되어 뇌척수액을 뽑아 그 뇌척수액으로 세균검사를 늦게 할 수 있습니다.
이때 세균 배양 검사에 세균이 잘 자라지 않을 수 있습니다. 그래서 박테리아 뇌막염을 앓고 있는지 바이러스성 뇌막염을 앓고 있는지 또는 다른 원인으로 생긴 뇌막염을 앓는지 확실히 감별 진단할 수 없는 때도 있습니다.
항생제는 바이러스성 뇌막염 치료에 효과가 없습니다. 헤르페스바이러스성 뇌막염 및, 또는 뇌염이나 그 외 몇 가지 바이러스성 뇌막염 등을 치료할 수 있는 항 바이러스제가 있지만 대부분의 바이러스성 뇌막염은 대증 치료를 하는 것이 거의 입니다.
바이러스성 뇌막염으로 전신 경련을 한다든지 탈수가 심하게 되지 않을 때는 박테리아 뇌막염에 걸리지 않았다고 진단을 한 후 병원에서 치료하는 것보다 집에서 부모들이 직접 치료하는 것이 일반적입니다.
홍역 바이러스, 에코콕삭키바이러스, 아데노바이러스, 멈프스바이러스, 일본뇌염바이러스 등 여러 종류의 바이러스가 바이러스성 뇌염 및, 또는 바이러스성 뇌막염을 일으킬 수 있습니다.
뇌염 및, 또는 뇌막염을 일으킨 바이러스의 종류에 따라 병의 진행과정이 다르고 그때그때 증상 징후와 중증도가 다릅니다.
따라서 어떤 바이러스 감염에 의해서 생긴 뇌막염을 앓고 있는지 저도 모릅니다.
뇌척수액 검사에는 단백질, 포도당, 백혈구 수, 백혈구 감별계산, 적혈구 수, 백혈구의 종류, 바이러스, 박테리아, 곰팡이, 기생충, 결핵균 등 세균검사와 혈청검사 등이 있습니다.
이런 검사 결과를 알아야 어떤 종류의 뇌막염 및, 또는 뇌염을 앓고 있는지 답변을 더 정확히 해드릴 수 있습니다.
결론을 내리면 하신 질문에 확답을 드릴 수 없습니다.
아기의 소아청소년과 의사에게 이런 질문을 확실히 하시는 것이 바람직스럽습니다.
뇌염, 뇌막염(수막염) 등을 참조하시기 바랍니다.
소아청소년과에서 진찰 진단 치료를 받고 상담하시기 바랍니다.
질문이 더 있으시면 다시 연락 주세요. 감사합니다. 이상원 드림
Meningococcal meningitis and Meningococcal septicemia, skin rashes
수막구균 뇌막염(수막구균 수막염)과 수막구균 패혈증, 피부 발진
Causes of meningococcal meningitis
Figure 2-64. It can be diagnosed by seeing the presence of meningococcus in leukocytes: a-meningococcus in leukocytes. Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
• Meningococcus (Neisseria meningitidis) is a type of bacteria and is called meningococcus.
• Meningococcal meningitis is an infectious disease caused by meningococcal infection.
• Meningococcal meningitis is a type of bacterial meningitis).
• Here, for convenience, meningococcal meningitis is referred to as “meningitis”.
• Meningococcal sepsis is an infectious disease in which meningococcal infection spreads throughout the body and causes systemic meningococcal inflammation.
Table 2-4. When the meninges are infected with meningococcal, the following meningococcal infectious diseases can occur. 표 2-4.수막구균에 수막(뇌막)이 감염되면 다음과 같은 수막구균 감염병이 발생될 수 있다.
| Type of infectious disease | incidence % |
| Meningitis | 47% |
| Meningococcal sepsis | 43% |
| Pneumonia | 6% |
| Other | 3.4% |
source; Rosenstein NE, et al. J Infect Dis. 1999; 180:1894-1901
• Acute fulminant meningococcal sepsis
• epiglottis
• otitis media
• conjunctivitis
• purulent arthritis
• purulent pericarditis
• chronic meningococcal sepsis.
• Healthy children and adults may have meningococcal in the pharyngeal or nasal mucosa, but meningococcal meningitis or meningococcal sepsis is not common.
• It is not clear why some people may develop meningococcal meningitis or meningococcal sepsis, while others do not develop meningococcal meningitis or meningococcal sepsis.
• Meningococcal infection can occur in others through saliva, sputum, or droplets containing meningococcal when a person with the disease breathes or speaks.
• People of all ages can develop this disease. However, it is more likely to develop in infants 6 to 12 months of age.
• It can only develop in healthy children who do not have any disease, but it may be more prevalent in children with colds or other types of viral upper respiratory tract infections.
• After 2-4 days of upper respiratory tract infection, meningococcal infection can lead to meningococcal meningitis and/or meningococcal sepsis.
• This disease is more likely to occur in military personnel, adults, children and adolescents living in groups such as school or daycare centers.
• The incubation period is 1-10 days.
Symptoms, signs of meningococcal meningitis
Figure 2-65. Meningococcal meningitis can cause systemic bleeding spots. Source; Used with permission from Ross Laboratories, Columbus, Ohio, USA
• Symptoms and signs of meningococcal meningitis vary.
• Symptoms and signs vary greatly from time to time.
• Typical symptomatic signs are:
• After meningococcal infection in the body, he suffers for 1 to 2 days, similar to a cold, then suddenly develops symptoms of life-threatening toxic conditions such as high fever and headache.
• You are immediately put into a toxic state. Very rarely, you may get mildly ill while moaning for several days.
• When meningococcal meningitis occurs, it is common to have a sudden, high fever and life-threatening illness.
• Meningococcal sepsis and/or meningitis may develop rapidly and spread throughout the body within a few hours after infection.
• Meningococcal sepsis and/or meningitis can lead to exhaustion, loss of strength, sagging, abnormal sleep, and systemic convulsions.
• Symptoms such as severe headache, chills, vomiting, systemic malaise, and joint pain may persist, and bleeding spots of various sizes may appear on the skin and mucous membranes (see Figure 2-65).
• [Parents should also be at least half doctors-Pediatrics and Family Nursing Encyclopedia]-Volume 17 Children and adolescents skin disease-Petichea hemorrhage on the head and face, skin rash (fever) and fever See meningococcal sepsis.
• Sometimes whole-body bleeding occurs, causing blood to form and bleeding spots on the entire skin and mucous membranes of the body.
• If this disease is diagnosed early and not actively treated, it is common to die within a short period of time.
Diagnosis of meningococcal meningitis
Figure 2-66. If encephalitis or meningitis is suspected, cerebrospinal fluid is drawn with a lumbar puncture and examined. Copyright ⓒ 2013 John Sangwon Lee, M.D. FAAP
• If this disease is suspected by taking the medical history, symptoms, signs, and examination findings together, the specimens are collected from blood, cerebrospinal fluid, urine, skin rash, etc., and a Gram-stained microscopic meningococcal bacterial test and bacterial culture test are performed.
• Diagnosis can be performed by testing for agglutination of meningococcal antigen antibodies with urine, blood, and cerebrospinal fluid.
• In general, when you can diagnose the disease by combining the symptoms and examination findings caused by the disease, it is often in a state of advanced disease that is life-threatening.
Treatment of meningococcal meningitis
• This disease really needs to be treated as an emergency during an emergency.
• If you suspect you have the disease, you should collect blood, cerebrospinal fluid, or other appropriate specimens as soon as possible, as soon as possible, as an emergency, to do a bacterial test that could be the cause of your hospital admission procedures for immediate treatment.
• At the same time, penicillin or other appropriate antibiotic vascular injection should be started immediately.
• Also, start treatment with blood glucose electrolyte solution vascular injection, and treat symptomatic according to the symptoms that occurred at that time.
• If the child is allergic to penicillin, emergency treatment is initiated with intravascular injection of Chloramphenicol, Cefotaxime, or another appropriate antibiotic.
• Depending on the time and location, it may be necessary to provide emergency treatment by intravenous vascular injection of antibiotics before collecting the specimen for bacteriological testing.
A procalcitonin test is used to differentially diagnose aseptic meningitis (aseptic meningitis) and bacterial meningitis.
In case of contact with the patient
• Prophylactic antibiotics with antibiotics such as oral rifampin to prevent adults, children and adolescents, their families, doctors, and nurses from getting the disease in close or in contact with a child with meningococcal meningitis and/or meningococcal sepsis. You need treatment.
• Children no longer need to be isolated 24 hours after the disease has been properly treated with appropriate antibiotics.
Meningococcal Infection Immunization for Infectious Diseases
Due to Meningococcal Infection
• Refer to the following pediatric and adolescent infectious disease vaccination schedule recommendations.
• Meningococcal infection can cause meningococcal meningitis, and the meningococcal can infect whole body blood and cause meningococcal sepsis.
• Sometimes meningococcal meningitis and meningococcal sepsis can occur simultaneously.
• There are 13 serogroups of meningococcal. Most of the meningococcal invasive infections are caused by groups A, B, C, Y, and W-135.
• There is a meningococcal vaccination vaccine that can prevent meningococcal infection in the A, C, Y, and W-135 serogroups.
Meningococcal vaccination vaccines include MPSV4 vaccine and MCV4 vaccine. However, there is no vaccination vaccine that can prevent meningococcal infection in the B serum group.
• The MPSV4 vaccine can be given by subcutaneous injection and can be vaccinated in children 2 to 10 years old with anatomical or functional non-spleen, or with end-stage complement deficiency.
• The MCV4 vaccine can be given intramuscularly and can be vaccinated against people aged 11 to 55 years old. However, the MCV4 vaccine can also be given to children aged 2-10 with health problems in high-risk groups.
• Infectious diseases caused by meningococcal infection can occur in children and adolescents and adults, and are more likely to occur in children and adults who live in groups such as military, school, or day care centers. Recently, it is recommended to include it in the basic vaccinations that can be given to adolescent children aged 11-12 years or older.
• Invasive meningococcal infection affects 2200 to 3,000 Americans a year, with 0.9 to 1.5 of 100,000 infants, 1.8 of 2 to 4 years old, 5 in the preschool, preschool, and adolescent age groups. There are studies showing that it occurred in 0.7 of children aged ~17 and 0.7 of young adults aged 18 to 34.
• There have often been instances of parents with children who have recovered or died from severe illness from an invasive meningococcal infection, unaware of the availability of a vaccine to prevent the disease. Therefore, parents should be informed that these vaccinations are available (see Tables 1 and 2). MPSV4 vaccine and MCV4 vaccine
• There are two types of meningococcal vaccines that can prevent infectious diseases caused by meningococcal infections belonging to the A, C, Y and W-135 serogroups of meningococcal. That is, there are the MPSV4 vaccine and MCV4 vaccine (see Table 1 and Table 2).
• MPSV4 vaccine (Meningococcal polysaccharide vaccine 4) is an abbreviation for meningococcal polysaccharide vaccine 4.
The MENOMUNE-A/C/Y/W-135 vaccine is the trade name of the MPSV4 vaccine. The MPSV4 vaccine is recommended to be given to infants aged 2 years and older, but the American Academy of Pediatrics and Adolescents recommends that the vaccine is given only to children with health problems belonging to high-risk groups who are highly susceptible to meningococcal infection.
• MCV4 vaccine stands for Meningococcal conjugate vaccine. The MCV4 vaccine is recommended to be vaccinated in children and adolescents aged 2 to 10 years of age in the high-risk group with a high risk of terminal complement deficiency, anatomical or functional non-spleen, or meningococcal infection. The MPSV4 vaccine can be used instead of the MCV4 vaccine.
• Infectious diseases caused by meningococcal infection can occur in children and adolescents or in adults at any time. However, it may be more prevalent in children and adolescents or adults living in groups such as military, school, or day care centers. How to inoculate
• If you have a fever after a medical examination, have a fever, check your body temperature, do not have a febrile infection, are not allergic to MCV4 vaccine or MPSV4 vaccine, and there are no contraindications for receiving the vaccine, you will receive the first dose. Inoculation effect
• The immune system that can be prevented appears 10-14 days after receiving the first vaccination.
• Research shows that children aged 2 to 4 years old have an immune effect of about 67% at 3 years after receiving group A meningococcal vaccination. In the following cases, they are especially vaccinated with a meningococcal infectious disease vaccine.
• The CDC in the United States has recommended routine vaccinations for all healthy children 11 years of age and older to prevent meningococcal infection since 2005.
• Children over 2 years of age with no spleen or abnormal spleen function
• For children 2 years of age or older with immune system deficiency, or for people with congenital or acquired Complement (complement) deficiency.
• For people who travel to regions or countries where meningococcal infectious diseases are prevalent.
• When this disease occurs in the area where you live
• For recruits and college students, especially freshmen living in dorms.
• To people who work in hospital clinical laboratory • To children and adolescents of parents who require vaccination
• etc
Vaccination age
• MPSV4 (MENOMUNE-A/C/Y/W-135) vaccine is not given to infants under 2 years of age. • It is not recommended that all healthy children and adolescents be vaccinated against meningococcal infection.
• Nevertheless, any child or adult in the age range of 11 to 70 can be vaccinated.
• In particular, it is recommended that adolescent children 11-12 years of age or older receive the meningococcal vaccination. Contraindications to vaccination Children and adolescents, adults, and pregnant women allergic to meningococcal vaccine or with a febrile infection are not eligible. Vaccination side effects
• Pain, redness, and swelling may occur in the area where the vaccine was injected. Rarely, an allergic reaction can occur.
• For more information, please visit www.vaccineshoppe.com.
•www.drleepediatrics.com
-Vol. 2 Prevention of pediatric and adolescent diseases and accidents. See the pediatric and adolescent vaccination schedule recommended by the US CDC in January 2015, the Society of Micro and Adolescents. Recommended immunization schedule for 0-18 year old Americal children in Jan 1st, 2013 ☞ The recommended basic vaccination schedule may differ depending on each country.
Recommended after January 2021 Basic vaccination schedule and table 1A for children and adolescents aged 0-18
Recommended immunization schedule for persons aged 0 through 18 years since
January 2021, 2021년 1월 이후 권장 미 0~18세 소아청소년 기본 예방접종 스케줄과 표 1A
Vaccination type of vaccine/ infectious disease that prevent
| Vaccination type of vaccine/ infectious disease that prevent | Right after birth | After birth 1 month | After birth 4 month | After birth 6 month | After birth 9 month | After birth 12 month | After birth 1 5 month | After birth 18 month | After birth 19~23 month | After birth 2-3 years old | After birth 4-6 years old | After birth 7-10 years old | After birth 11-12 years old | After birth 13-15 years old | After birth 16-18 years old | |||||||
| Hepatitis B¹ (HepB) /b 형 간염 | ←1st vaccination→ | ←2nd vaccination→ | ←←3rd vaccination→→ | |||||||||||||||||||
| Rotavirus² (RV) RV-1 (two batch sequence inoculation); RV-5 (3-batch sequence vaccination)/ Rotavirus infection | ←1st vaccination→ | ←2nd vaccination→ | note 2 | |||||||||||||||||||
| Diphtheria, Tetanus, acellular Pertussis³ (DTaP; <7 years old)/tetanus, diphtheria, pertussi | ←1st vaccination→ | ←2nd vaccination→ | ←3rd vaccination→ | ←4th vaccination→ | ←5th vaccination→ | |||||||||||||||||
| Tetanus, Diphtheria, acellular Pertussis⁴ (DTap; 7 years old> 7 years old tetanus, diphtheria, whooping cough | (Tdap) | |||||||||||||||||||||
| Haemophilus influenzae type b⁵(HIb)/ Hib infectious disease | ←1st vaccination→ | ←2nd vaccination→ | note 5 | ←3rd or 4th vaccination→ Footnote 5 | ||||||||||||||||||
| Pneumococcal conjugate⁶a, c (PCV13)/Pneumococcal infection | ←1st vaccination→ | ←2nd vaccination→ | ←3rd vaccination→ | ←4th vaccination→ | ||||||||||||||||||
| Pneumococcal polysaccharide⁶bc (PPSV23) / Streptococcal pneumonia infection | ||||||||||||||||||||||
| Inactivated Poliovirus⁷(IPV)(<18 years old)/Polio | ←1st vaccination→ | ←2nd vaccination→ | ←3rd vaccination→ | ←4th vaccination→ | ||||||||||||||||||
| Vaccination type of vaccine/ infectious disease that prevent | Right after birth | After birth 1 month | After birth 2 month | After birth 4 month | After birth 6 month | After birth 9 month | After birth 12 month | After birth 15 month | After birth 18 month | After birth 19-23 month | After birth 2-3 years old | After birth 4-6 years old | After birth 7-10 years old | After birth 11-12 years old | After birth 13-15 years old | After birth 16-18 years old | ||
| Influenza⁸ (IIV; LAIV) for 1 copy, 2 servings, footnote 8 / Influenza | ←Get inoculated every year (11V 만)→ | ←Get inoculated every year(II V or LAIV)→ | ||||||||||||||||
| Measles, Mumps, Rubella⁹(MMR)/ Measles, Rubella, Mumps | ←1st vaccination→ | ←2nd vaccination→ | ||||||||||||||||
| Varicella ¹⁰ (VAR) /Varicella | ←1st vaccination→ | ←2nd vaccination→ | ||||||||||||||||
| Hepatitis A¹¹ (HepA)/Hepatitis A | ←2 doses→ | |||||||||||||||||
| (Human papillomavirus¹² (HPV2; women only (HPV4; women and men))/Human papillomavirus infectious disease | ←3rd vaccination→ | |||||||||||||||||
| Meningococcal¹³ (MenACWY-D 9 months or later. MenACWY-CRM-D is 2 months or later. MenACWY-TT is 2 years old or later. / Meningococcal meningitis and other infectious diseases) —————————- Meningococcal B vaccines include MenB-4C, Bexsero, MenB-FHbp, and Trumenba vaccines. We touch on 10 years of age or older. The Bexsero vaccine is inoculated twice and the Trumenba vaccine has been inoculated a total of three times. Adolescents and young adults with no risk are vaccinated at age 16-23. Source: CDC, AAP News 3/2021 | ←1st vaccination→ | Booster vaccination | ||||||||||||||||
|
|
The age range for which vaccination is recommended, | ||
|
|
Age recommending vaccination for children in the high risk group |
Differential diagnosis of aseptic meningitis and bacterial meningitis
• Meningitis caused by a viral infection of the meninges, non-bacterial pathogen infections of the meninges, or heavy metal poisoning of the meninges is called aseptic meningitis.
• Bacterial meningitis is meningitis caused by a bacterial infection.
• CBC blood test, other blood test, C-reactive protein blood concentration, and quantitative test of procalcitonin (PCT) are usefully used to diagnose infectious diseases. • Among them, the procalcitonin quantitative test is said to have the most useful diagnostic value.
• Procalcitonin is a precursor to the hormone calcitonin and is produced in the C cells of the thyroid gland. Procalcitonin is not secreted in the blood of a normal healthy person.
• In severe systemic infectious diseases, blood levels of procalcitonin may be increased to 100ng or more.
• 5% of children’s meningitis (meningitis) is bacterial meningitis and the remainder is aseptic meningitis.
• When children have meningitis, it is common to perform a quantitative test for procalcitonin, C-reactive protein, total white blood cell count, and neutrophil count from the blood, and to draw cerebrospinal fluid.
• It is common to differentially diagnose whether you have aseptic meningitis or bacterial meningitis by using protein concentration, glucose concentration, white blood cell count, neutrophil count, Gram staining microscopic bacterial examination, and bacterial antigen test in the cerebrospinal fluid.
• If the result of the quantitative procalcitonin test is abnormally increased among the various test results described above, it can be diagnosed as having bacterial (sex) meningitis.
• Therefore, this test is very important when you have meningitis.
The following is an example of the Internet pediatric and adolescent health counseling question and answer on “meningitis”.
Q&A.
About meningitis
Q.
Good morning. My child had meningitis and was treated for two weeks before being discharged on September 14th. But on September 19th, when I went to the hospital because of a fever, they said it was meningitis.
Can you do that in less than a week?
The hospital said that when discharged, there were only 3 inflammatory cells when the spinal cord was examined. He said that all children have that much. What are the preventive measures or vaccinations?
A.
Sumi Good morning. Thanks for the great question.
The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided. Meningitis (meningitis) can also result from a meningeal virus infection, a meningeal bacterial infection, or other meningeal pathogen infection.
Rarely, a non-pathogenic infection can result in meningitis due to chemical toxicity to the meninges or leukemia and malignant cell invasion.
Depending on what causes meningitis, symptoms, signs, diagnosis, treatment, etc. are different, and the prognosis is very different. If you let us know what kind of bacteria or virus infection has caused meningitis, we can give you a more reliable answer. Meningitis that was incompletely treated may recur, or new meningitis may come back from another bacterial infection.
Rarely, there is an abnormal fistula between the nasal cavity and the meninges, or some congenital malformations are connected to the meninges, and bacteria may infect the meninges (meninges) through the connected passages, causing meningitis to recur. This is practically very rare. Meningitis may recur when the resistance to bacterial infection is weak or absent due to leukopenia or immune system deficiency. Sometimes meningitis is not completely cured, and treatment may be stopped shortly after treatment is stopped, and meningitis may recur. This is called partially treated meningitis. It is also important to do a cerebrospinal fluid test and a CT scan of the brain to see if there is an abscess in the brain.
Please continue to receive treatment from your baby’s regular pediatrician and consult with your doctor. www.drleepediatrics.com-Volume 2 Prevention of pediatric and adolescent diseases and safety accidents-Meningococcal vaccination, See meningitis, etc. Please consult with the Department of Pediatrics and Adolescents after receiving medical examination and treatment. If you have more questions, please contact us again. Thank you. Lee Sang-won. MD
The following is an example of an Internet pediatric and adolescent health counseling question and answer for “Additional Meningitis Question…”. Q&A. Meningitis additional question…
Q.
Thank you for your kind answers even while you’re busy. I have a more specific question, so I am writing a few words. My son, who had meningitis, is now 4 months old. When he was first admitted to the hospital, he said he had 95 inflammatory cells. He fell to 3 after about 12 days of treatment and was discharged at the 2nd week.
At that time, he found that there was no abnormality in brain MRI scans and blood and urine tests as a result of viral meningitis. But what I’m curious about is that the number of inflammatory cells has increased to 12 within a week of being discharged (about 5 days).
Even in children and adolescents with weak immunity, is meningitis as easy as a cold and recurs easily? I wonder if the hospital has neglected treatment or discharged a child who has not yet been cured. I wrote not about the hospital’s negligence, but to make sure that the same thing does not cause my child to suffer twice. Then, good luck.
A.
Sumi Good morning. Thank you for asking another good question.
The more information you know about your child’s age, gender, past medical history, family medical history, medical examination findings, and clinical examination, the more helpful it is to give you an answer. We will respond based on the information you provided.
Now you can know a little more about what kind of illness you had. Thanks for more information. When you first asked, we answered without knowing if you had viral meningitis and/or viral encephalitis, bacterial meningitis, or meningitis from other causes.
It’s not clear right now if your baby has any other type of bacterial meningitis, viral meningitis, and/or encephalitis, or if a previous encephalopathy has recurred or if you are worried about the natural course of the disease.
There is also a way to know for sure what pathogens cause meningitis and/or encephalitis by viral culture or bacterial culture with cerebrospinal fluid, meninges, or samples obtained from the brain. Typically, cerebrospinal fluid is not tested for virus cultures a lot.
If the bacteria are not cultured in the cerebrospinal fluid culture test, it is customary to diagnose meningitis as a result of a viral infection. In the past, when patients bought antibiotics at their own discretion at pharmacies and treated their own diseases, parents said that children suffering from bacterial meningitis had a cold. And bacterial meningitis developed chronically.
That chronic bacterial meningitis recurred again as acute meningitis. It is common in pediatrics and adolescents to do a cerebrospinal fluid test when a high fever occurs without a clear cause.
Before the cerebrospinal fluid is tested, it is diagnosed that there is an infectious disease other than meningitis, and the infectious disease is incompletely treated with antibiotics, and it is suspected that you have bacterial meningitis.
At this time, the bacteria may not grow well in the bacterial culture test.
So there are times when it is not possible to make a distinction between having bacterial meningitis, viral meningitis, or meningitis from other causes. Antibiotics are not effective in treating viral meningitis. There are antiviral drugs that can treat herpesviral meningitis and/or encephalitis or some other viral meningitis, but most of the viral meningitis is treated as symptomatic. When viral meningitis causes systemic convulsions or dehydration does not become severe, it is more common for parents to treat themselves at home rather than at a hospital after being diagnosed with bacterial meningitis. Several types of viruses can cause viral encephalitis and/or viral meningitis, such as measles virus, ecocoxaki virus, adenovirus, mumps virus, and Japanese encephalitis virus.
Depending on the type of virus that caused encephalitis and/or meningitis, the course of the disease is different, and the symptoms and symptoms are different from time to time.
So I don’t know what kind of viral infection I have meningitis. Cerebrospinal fluid tests include protein, glucose, white blood cell count, white blood cell differential count, red blood cell count, type of white blood cell, bacterial tests such as viruses, bacteria, fungi, parasites, and Mycobacterium tuberculosis, and serum tests. Knowing the results of these tests can give you more accurate answers about what types of meningitis and/or encephalitis you have. When we come to a conclusion, we cannot give a definite answer to the question you asked. It is advisable to make these questions clear to your baby’s pediatrician. Please refer to encephalitis, meningitis (meningitis), etc.
Please consult with the Department of Pediatrics and Adolescents after receiving medical examination and treatment. If you have more questions, please contact us again. Thank you. Lee Sang-won. MD
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Nelson Textbook of Pediatrics 14th ed. Beherman,
-
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th edition 2012
-
Nelson Text Book of Pediatrics 19th Edition
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 안효섭 외 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”