소화성 궤양 Peptic ulcer diseases
소화성 궤양의 개요
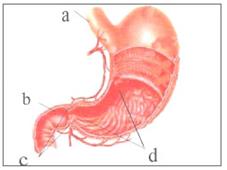
그림 208. 위 해부도
a-식도, b-유문, c-유문 괄약근, d-위 벽
출처; Used with permission from Glaxo Wellcome
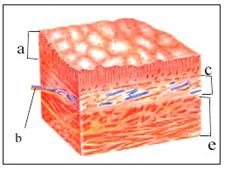
그림 209. 위 벽의 조직
a-점막층, b-혈관, c-점막층하 조직층, d-근육층, e-장막층
출처; Used with permission from Glaxo Wellcome
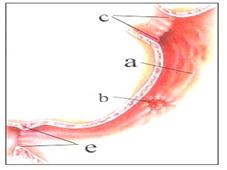
그림 210. 소화성 위궤양
a-위벽, b-소화성 위궤양, c-분문, e-유문
출처; Used with permission from Glaxo Wellcome과 소아가정간호백과
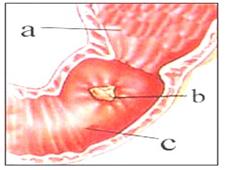
그림 211. 십이지장 궤양(소화성 십이지장 궤양)
a-위벽, b-소화성 십이지장 궤양, c-십이지장의 장벽
출처; Used with permission from Glaxo Wellcome과 소아가정간호백과
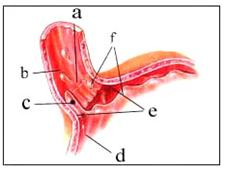
그림 212. 위 식도 역류
a-위 식도 경계, b-식도 벽, c-위액의 역류, d-위벽, e-분문, f-위액
출처; Used with permission from Glaxo Wellcome과 소아가정간호백과
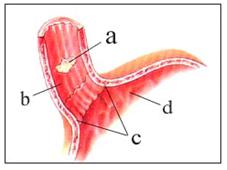
그림 213. 식도 소화성 궤양
a-궤양, b-식도 벽, c-분문, d-위 벽
출처; Used with permission from Glaxo Wellcome과 소아가정간호백과
-
위, 십이지장, 또는 식도 하단 점막층이 위산과 펩신 등 위액에 노출될 때 위나 십이지장 등의 점막층이 둥글게 헐고 짓무르며 마치 화산 분화구 모양처럼 위, 십이지장, 또는 식도의 벽이 손상되는 위장관 병을 소화성 궤양이라고 한다.
-
소화성 궤양이 위 벽에 생기면 소화성 위궤양, 십이지장에 생기면 소화성 십이지장 궤양이라고 하고 식도 벽에 생기면 소화성 식도 궤양이라고 한다.
소화성 궤양의 원인
-
여기서는 편의상 소화성 위궤양을 위궤양, 소화성 십이지장 궤양을 십이지장 궤양이라고 칭한다.
-
위궤양이나 십이지장 궤양의 원인은 아직도 확실히 모른다.
-
친 부모 형제자매들 중 누군가가 위궤양을 앓았던 병력이 있으면 그들의 다른 형제자매들 중 누군가가 위궤양에 걸릴 가능성이 더 많다.
-
O형 혈액형을 가진 소아청소년들, 스트레스를 많이 받는 아이들은 위궤양에 더 잘 걸릴 수 있다고 한다.
-
단백질을 소화시키는 관련되는 펩신과 위산, 그밖에 다른 종류의 위액의 성분으로 위 벽 점막층이나 십이지장 벽 점막층 또는 식도 벽 점막층 등이 국소적으로 손상될 때 위궤양이나 십이지장 궤양 또는 식도 궤양이 생길 수 있다.
-
따라서 펩신과 위산 등 위액에 접촉될 수 있는 위, 십이지장, 식도 하단부 등에 소화성 궤양이 생길 수 있다.
-
소장관 벽 조직의 일부에 위 벽 점막층이 엉뚱하게 조금 끼어 있을 수 있다. 이런 점막층을 이소성 위 점막층이라고 한다.
-
이소성 위 점막층이 있는 소장관 벽 일부에 소화성 궤양이 생길 수 있다.
-
소화성 위궤양이나 소화성 십이지장 궤양이 생긴 위 벽 점막층이나 십이지장 점막층은 붓고 헐고 짓무른다. 그 궤양이 점점 더 악화되면 궤양이 생겨 있는 점막층 뿐만 아니라 궤양이 있는 점막층의 바로 밑에 있는 점막층 하 조직, 그 하 조직 아래에 있는 근육층이 손상될 수 있다.궤양으로 점막층과 근육층이 손상되고 그 귀양 환부가 점점 더 퍼져갈 때 마지막으로 궤양이 생긴 위벽이나 십이지장의 장벽에 있는 혈관이 파열될 수 있다. 이럴 때 위궤양이나 십이지장 궤양이 있는 장벽에서 피가 날 수 있다.
-
거기서 피가 대량으로 날 때 피를 토하거나 빨간 피가 항문으로 나올 수 있다. 더 나아가서 위벽이나 십이지장벽의 전체 층이 천공될 수 있다.
|
요약하면 소화성 위궤양이나 소화성 십이지장 궤양이 생긴 위 벽 점막층이나 십이지장 벽 점막층이 붓고 헐고→점막층 하 조직이 붓고 헐고→근육층이 손상되고→위벽이나 십이지장의 장벽에 있는 혈관이 파열→위벽이나 십이지장의 장벽의 파열 |
-
헬리코박터 파일로리균 감염으로 소화성 위궤양이 생길 수 있다.
-
p.00 위궤양이나 십이지장 궤양으로 갑자기 배가 아플 때 참조.
소화성 궤양의 증상 징후
-
소화성 위궤양이나 소화성 십이지장 궤양의 증상 징후는 나이, 중증도, 위궤양이나 십이지장 궤양의 합병증의 유무 등에 따라 다르다.
-
전형적인 증상 징후는 다음과 같다.
-
나이가 어릴수록 위궤양이나 십이지장 궤양의 증상 징후가 뚜렷하게 나타나지 않는 것이 보통이다.
-
학령기 아이들이나 사춘기 아이들에게 위궤양이나 십이지장 궤양이 생기면, 식사를 하기 바로 전과 식사 후 2∼3시간 경에 오목가슴이나 배꼽 부위나 배 전체가 쓰리고 아플 수 있다.
-
음식물을 먹는 시간과 관계없이 배가 아플 수 있다.
-
위나 십이지장에 소화성 궤양이 있지만 아무 증상 징후가 없을 수 있다.
-
드물게는 구토하기도 한다.
-
때로는 궤양이 있는 위나 십이지장의 벽 국소에서 피가 대량으로 나 그 피를 토하거나 피똥을 누기도 한다.
-
궤양이 있는 위장관 벽이 뚫려 위나 십이지장의 벽에 천공이 생기고, 출혈하고, 쇼크에 빠질 수 있다.
-
어떤 때에는 앞서 설명한 여러 가지 증상 징후 중 한두 가지 증상 징후만 있어서 병원에 갔다가 소화성 위궤양을 우연히 처음 진단 받을 때도 있다.
-
드물게 위나 십이지장의 소화성 궤양으로 인해 위나 십이지장관이 막힐 수 있다.
-
학령기 전 유아들이나 학령기 아이들, 사춘기 아이들의 위궤양이나 십이지장 궤양의 증상 징후는 성인들의 소화성 위장 궤양이나 소화성 십이지장 궤양의 증상 징후가 거의 비슷하다.
-
오목가슴이나 배꼽 주위, 아랫배, 또는 배 전체가 아무 때나 불규칙하게 아플 수 있다.
-
어떤 때는 며칠 동안, 또는 몇 주일 동안 조금도 아프지 않다가 아픈 증상이 재발될 수 있다. 합병증이 없으면 대부분 3∼8주 동안 적절히 치료하면 잘 낫는다.
-
그러나 재발될 수 있다.
소화성 궤양의 진단
-
병력·증상 징후·진찰소견 등을 종합하여 소화성 궤양이 있다고 의심되면 경구로 조영물을 먹은 후 식도·위·십이지장 X-선 사진검사 등으로 진단할 수 있으나 위장 X-선 사진 검사로 확실히 진단할 수 없는 때가 있다.
-
혈액·소변·대변 검사를 한다. 특히 대변에 잠복혈이 나오나 검사해 본다.
-
특수 거울이 달린 위장내시경을 위 속과 십이지장관 속에 넣고 위장 내시경을 통해 위와 십이지장관 벽 점막층을 육안으로 직접 보고 진단한다.
-
식도염·위염·췌장염 및 담관에 생긴 여러 종류의 병, 위장관 기생충증, 충수염, 중금속 중독, 그밖에 다른 병이 있을 때도 위나 십이지장 궤양의 증상 징후와 거의 비슷한 증상이 생길 수 있다. 그런 병들과 감별·진단해야 한다.
소화성 궤양의 치료
-
아직도 위궤양이나 십이지장 궤양을 100% 완치할 수 있는 치료 방법이 없다.
-
일반적으로 내과적으로 치료한다.
-
위산 농도를 감소시키기 위해서 알루미늄 하이드로옥사이드제(Aluminum hydroxide)나 마그네슘 트리실리케이트제(Magnesium trisilicate), 또는 칼슘 카보네이드제(Calcium Carbonate) 중 한두 가지의 제산제나 종합 제산제로 우선 치료한다. 액체 제산제가 정제 제산제보다 효과가 더 좋다고 한다. 제산제의 용량은 나이와 궤양의 중증도에 따라 다르다. 제산제를 복용하는 시간도 제산제 종류와 증상에 따라 다르다. 매 식사 후 1∼2시간 되었을 때와 잠자기 바로 전에 1회, 하루에 4회 복용하는 것이 보통이다.
-
프로반딘 부교감신경 작용 차단제를 1일 1회 자기 전에 복용할 수 있다.
-
의사의 처방에 따라 시메티딘(Cimetidine)이나 잔탁(Zantac) 또는 가스터(Gaster)제 중 한 가지 약물을 선택해서 3∼8주일 동안 치료해 주면 소화성 궤양 70∼80% 정도는 쉽게 낫는다.
-
시메티딘을 매 식사하기 30분 전과 자기 바로 전에 한 번 하루 두 번 복용한다.
-
균형 잡힌 영양 음식물을 섭취해야 한다.
-
커피·콜라·술 등 자극성 음식물은 소화성 궤양에 좋지 않은 음료수이다.
-
위궤양이나 십이지장 궤양으로 위장 출혈이 생기거나 위장 천공 등의 합병증이 있을 때에는 수술 치료를 한다.
-
헬리코박터 파일로리균 감염으로 소화성 궤양이 생길 수 있다. 이 균을 죽이기 위해선 아목시실린(Amoxicillin)과 메트로니다졸(Metronidazole/Flagyl)과 비스무스 서브샐리실에트 이 세 가지 약(3종 치료약)으로 치료한다.
-
헬리코박터 파일로리균 감염으로 생긴 성인 소화성 궤양은 Amoxicillin, Clarithromycin (Biaxin), Metronidazole (Flagyl) 와 Tetracycline으로 치료한다.
-
위산 분비를 감소시키고 궤양상처를 조기 치유하기 위해 Omeprazole (Prilosec), lansoprazole (Prevacid), Rabeprazole (Aciphex), Esomeprazole (Nexium) , Pantoprazole (Protonix) 중 한 가지를 선택해 치료할 수 있다.
-
3~12 세 이상 소아의 궤양을 치료할 때 Cimetidine (Tagamet), 12세 이상의 경우 Ranitidine (Zantac) 등 히스타민-2 수용체 길항제로 산 분비를 낮게 해 치료 할 수 있다.
-
Sulcralfate (Carafate)나 Misoprostol (Cytotec)으로 세포 손상을 보호하거나 bismuth subsalicylate (Pepto-Bismol)으로 치료한다.
Peptic ulcer diseases 소화성 궤양
Overview of peptic ulcer
Figure 208. Anatomy of the stomach a-esophagus, b-pylorus, c-pyloric sphincter, d-gastric wall source; Used with permission from Glaxo Wellcome
Figure 209. Organization of the upper wall a-mucosal layer, b-vascular, c-submucosal tissue layer, d-muscular layer, e-seous layer source; Used with permission from Glaxo Wellcome
Figure 210. Peptic gastric ulcer a-gastric wall, b-peptic gastric ulcer, c-cardial, e-pylorus source; Used with permission from Glaxo Wellcome Department of Pediatric Home Nursing
Figure 211. Duodenal ulcer (peptic duodenal ulcer) a-gastric wall, b-peptic duodenal ulcer, c-barrier of the duodenum source; Used with permission from Glaxo Wellcome Department of Pediatric Home Nursing
Figure 212. Gastroesophageal reflux a-gastric esophageal border, b-esophageal wall, c-regurgitation of gastric juice, d-gastric wall, e-cardial, f-gastric juice source; Used with permission from Glaxo Wellcome Department of Pediatric Home Nursing
Figure 213. Esophageal peptic ulcer a-ulcer, b-esophageal wall, c-cardiac, d-gastric wall source; Used with permission from Glaxo Wellcome Department of Pediatric Home Nursing
• When the mucous membrane of the stomach, duodenum, or the lower esophagus is exposed to gastric juices such as gastric acid and pepsin, the mucous membranes of the stomach or duodenum are rounded and crushed. It is called.
• If a peptic ulcer occurs on the wall of the stomach, it is called a peptic gastric ulcer, and if it occurs on the duodenum, it is called a peptic duodenal ulcer. If it occurs on the wall of the esophagus, it is called a peptic ulcer.
Causes of peptic ulcer
• Here, for convenience, peptic gastric ulcer is referred to as gastric ulcer, and peptic duodenal ulcer is referred to as duodenal ulcer.
• The cause of gastric or duodenal ulcers is still unknown. • If any of their parental siblings have a history of gastric ulcers, some of their other siblings are more likely to develop gastric ulcers.
• Children and adolescents with blood type O, and children under high stress, are said to be more susceptible to gastric ulcers.
• Locally injured gastric mucosa, duodenal mucosa, or esophageal mucosa with related pepsin and gastric acid and other gastric juices that digest proteins, can lead to gastric ulcer, duodenal ulcer, or esophageal ulcer.
• Therefore, peptic ulcer may develop in the stomach, duodenum, and lower part of the esophagus that may come into contact with gastric juices such as pepsin and gastric acid. • Part of the tissue in the small intestine wall may have a little bit of the mucous membrane of the stomach wall. This mucous layer is called the ectopic gastric mucosa. • A peptic ulcer may develop on a portion of the wall of the small intestine that contains the ectopic gastric mucosa.
• Peptic gastric ulcer or peptic duodenal ulcer, the mucous membrane of the stomach wall or the duodenal mucosa is swollen, loosened, and crushed. If the ulcer gets worse, the ulcer can damage not only the mucous membrane layer where the ulcer is formed, but also the submucosal layer underneath the ulcerous mucosa, and the muscle layer underneath the ulcer. As it spreads more and more, blood vessels in the last ulcerated stomach wall or in the duodenum’s barrier can rupture. This can lead to bleeding from the intestinal wall with a stomach ulcer or duodenal ulcer.
• When there is a large amount of bleeding, blood may vomit or red blood may come out of the anus.
Furthermore, the entire layer of the stomach or duodenum can be perforated. to summarize Peptic gastric ulcer or peptic duodenal ulcer swelling and tearing of the mucous membrane of the stomach wall or duodenal wall → swelling and tearing of the submucosal layer → muscle layer damage → rupture of blood vessels in the gastric wall or duodenum barrier → rupture of the gastric wall or duodenal barrier
• Helicobacter pylori infection can lead to peptic gastric ulcers.
• See Sudden stomach ache from a stomach or duodenal ulcer. Symptoms signs of peptic ulcer
• Symptoms of peptic gastric ulcer or peptic duodenal ulcer depend on age, severity, and the presence or absence of complications of gastric ulcer or duodenal ulcer.
Typical symptomatic signs are:
• The younger you are, the less obvious symptoms of gastric ulcer or duodenal ulcer are usually present.
• When school-age children or adolescent children have stomach ulcers or duodenal ulcers, the concave chest, navel area, or entire stomach may be sore and painful just before eating and 2-3 hours after eating.
• Regardless of the time you eat, your stomach can hurt.
• You have a peptic ulcer in your stomach or duodenum, but there may be no signs of symptoms.
• Rarely, vomiting occurs. • Occasionally, a large amount of bleeding occurs in the area of the wall of the stomach or duodenum where there is an ulcer, vomiting or bleeding.
• An ulcerated gastrointestinal wall can be punctured, resulting in perforation, bleeding, and shock in the wall of the stomach or duodenum.
• Sometimes, when you go to the hospital because of only one or two of the symptoms described above, you are accidentally diagnosed with a peptic ulcer for the first time.
• Rarely, a peptic ulcer in the stomach or duodenum can block the stomach or duodenum.
• Symptoms of gastric ulcer or duodenal ulcer in preschool infants, school-age children, and adolescent children are similar to those of peptic gastrointestinal ulcer or peptic duodenal ulcer in adults.
• The concave chest, around the navel, the lower abdomen, or the entire stomach may hurt irregularly at any time.
• Sometimes, symptoms may recur after not having any pain for days or weeks. If there are no complications, most of them will heal well with proper treatment for 3-8 weeks.
• However, it can recur.
Diagnosis of peptic ulcer
• If you suspect that you have a peptic ulcer by taking a summary of your medical history, symptoms, and examination findings, you can diagnose it with esophageal, gastric, and duodenal X-rays after taking a contrast material orally. There are times when you can’t.
• Blood, urine, and stool tests are done. In particular, examine the stool for latent blood.
• A gastrointestinal endoscope with a special mirror is placed in the stomach and duodenal canal, and the gastrointestinal endoscope is used to directly visually view and diagnose the mucous membrane of the stomach and duodenal tract.
• Esophagitis, gastritis, pancreatitis, and various diseases of the bile duct, gastrointestinal parasites, appendicitis, heavy metal poisoning, and other diseases can cause symptoms similar to those of gastric or duodenal ulcers. You must differentiate and diagnose such diseases.
Treatment of peptic ulcer
• There is still no cure for gastric or duodenal ulcers 100%.
• Generally treated medically.
• To reduce the concentration of gastric acid, first treatment with one or two antacids or synthetic antacids among aluminum hydroxide, magnesium trisilicate, or calcium carbonate. Liquid antacids are said to work better than refined antacids. The dosage of antacids depends on the age and severity of the ulcer. The amount of time you take antacids also depends on the type of antacid and your symptoms. It is common to take it 1 to 2 hours after each meal and just before bedtime, 4 times a day.
• Probandin parasympathetic blockers can be taken once a day before bed.
• According to your doctor’s prescription, if you choose one of Cimetidine, Zantac, or Gaster and treat it for 3 to 8 weeks, about 70-80% of peptic ulcers will be healed easily.
• Take cimetidine twice a day, 30 minutes before each meal and just before bedtime.
• Eat a balanced, nutritious diet.
• Irritating foods such as coffee, cola, and alcohol are not good for peptic ulcers. • If there is gastric bleeding due to gastric ulcer or duodenal ulcer or complications such as gastrointestinal perforation, surgical treatment is performed.
• Helicobacter pylori infection can lead to peptic ulcers. To kill the bacteria, they are treated with three drugs (three drugs): Amoxicillin, Metronidazole/Flagyl and Bismuth Subsalicilet.
• Adult peptic ulcers caused by Helicobacter pylori infection are treated with Amoxicillin, Clarithromycin (Biaxin), Metronidazole (Flagyl) and Tetracycline.
• To reduce gastric acid secretion and heal ulcer wounds early, Omeprazole (Prilosec), lansoprazole (Prevacid), Rabeprazole (Aciphex), Esomeprazole (Nexium), Pantoprazole (Protonix) can be selected for treatment.
• Histamine-2 receptor antagonists such as Cimetidine (Tagamet) and Ranitidine (Zantac) for children aged 3 to 12 years or older can be treated by lowering acid secretion.
• Protect cell damage with Sulcralfate (Carafate) or Misoprostol (Cytotec) or treat with bismuth subsalicylate (Pepto-Bismol).
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th-31st Ed 2021
-
Nelson Text Book of Pediatrics 19th-21st Edition
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”