성장 중지증(성장 부전/성장 실패/성장 장애) Failure to thrive
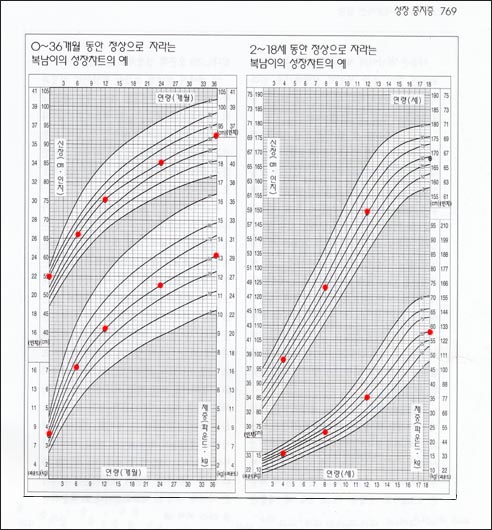
그림 5-6. 생후 0-36개월 동안 50백분위선을 따라 자라는 복남이의 성장차트의 예(좌)
2-18세 동안 50백분위선을 따라 자라는 복남이의 성장차트의 예(우)
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
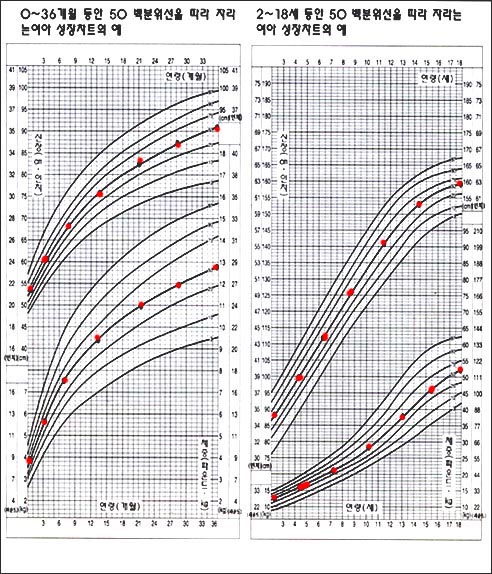
그림 5-5. 생후 0~36개월 동안 50 백분위선을 따라 자라는 신생아기, 영유아기의 여아 성장차트의 예(좌)
생후 2~18세 동안 50 백분위선을 따라 자라는 유아, 학령기, 사춘기의 여아 성장차트의 예(우)
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- 어린 영유 자녀를 소아청소년과로 데리고 와서 “내 아이는 밥도 잘 먹고 매일 달걀을 하나씩 먹고, 우유도 한 컵씩 마시고, 고기도 충분히 먹고 비타민을 하루도 빼놓지 않고 매일 먹는데 왜 잘 크지 않는지 모르겠다!” 호소면서 그 이유가 무엇인지 자세히 진찰해 알려 달라고 요구하는 부모들이 가끔 있다.
- “저 아이는 항상 핏기가 없고 창백하고 기운이 없는데 빈혈이 있는지, 또는 기생충증이 있는지 자세히 진찰해 달라”고 부탁하는 부모들도 가끔 있다.
- 그런 아이의 신장과 체중을 재고 머리끝서부터 발끝까지 자세히 진찰해 보고 CBC 피 검사, 소대변 검사를 비롯한 적절한 다른 검사를 해보면 빈혈도 없고 피, 소변, 대변 검사의 결과가 모두 정상이고 대변에 기생충 알도 성충도 없고 그 자녀는 정상적으로 적절히 잘 자라는 건강한 아이라고 평가할 때가 많다.
- 그 때 그 부모에게 그 자녀의 체중 치와 신장 치를 성장차트에 그려 체중 백분위선과 신장 백분위선을 보여 주면서 자녀의 체중은 자녀의 체중 백분위선을 따라, 신장은 자녀의 신장 백분위선을 따라 정상적 성장 속도로 계속 잘 자라고 있다는 것을 부모에게 보이고, 자녀의 성장에 관하여 잘 설명해 주면 부모는 자녀가 정상적으로 자라고 있다는 것을 이해하고 안심한다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제14권 소아청소년 내분비, 유전, 염색체, 대사, 희귀병 질환 참조.
- 거기다가 자녀가 그 간 자라왔던 성장 속도와 거의 같은 성장 속도로 앞으로도 계속 자라서 18세가 될 때의 추정 체중 치와 신장 치가 얼마나 될 것이라는 것도 설명해 주면 그 부모는 더 안도감을 갖는 것을 볼 수 있다.
- 드물게, 어떤 어린 영유 자녀가 그 동안에 섭취했던 음식물이 자녀의 체질에 맞지 않아 필요한 영양분과 칼로리를 충분히 섭취 못해서 정상적으로 체중이 증가되지 않고 성장 발육이 전체적으로 지연되어 있는 경우도 드물게 있다. 그러나 정기 건강검진 등으로 이런 현상은 요즘에는 아주 드물다.
- 어떤 질병으로 인해 체중이 나이에 비해 적절하게 증가되지 않을 수 있다. 때로는 성장이 비정상적으로 지연 내지 중지될 수 있다.
- 어떤 아이의 체중이 그 아이가 타고 난 성장속도에 따라 잘 증가하지 않거나 성장이 중지된 것 같으면, 그 원인을 찾기 위해 신체 검진을 받고 피·소변·대변 등 피검물로 적절한 임상 검사를 해서 그 원인을 규명해야 할 때도 있다.
- 소아 정기 건강검진을 주기적으로 해 주기 위해서 어린 영유아 자녀를 소아청소년과에 데리고 오기 전까지 그 자녀가 적절하게 잘 자라고 있다고 부모는 믿고 있었으나 소아청소년과에서 정기 건강검진을 받고 그 자녀가 적절하게 성장 발육되지 않는다는 것을 처음 진단 받을 때도 가끔 있다.
- 때로는 신장과 체중의 성장속도가 어떤 이유로 또래 아이들보다 비정상적으로 훨씬 느리지만 적절하게 잘 자라지 않아서 체구가 선천성으로 아주 작은 아이들도 있다. 그래서 성장 중지증이 있는 것같이 진단 받을 수 있다.
- 요약하면, 어떤 아이의 체중이나 신장의 성장 속도가 그 아이의 성별과 같은 동년배 아이들에 비해서 현저히 늦을 때 성장 중지증, 성장 부전, 성장 실패, 또는 성장 장애(Failure to thrive)라고 정의한다([부모도 반의사가 되어야 한다-소아가정간호백과]-제14권 소아청소년 내분비, 유전, 염색체, 대사, 희귀병 질환-키가 작은 아이 참조).
성장 중지증의 원인
1. 성장 중지증의 외적 원인
-
가난해서 음식물을 충분히 먹을 수 없을 때,
-
영양가가 거의 없는 음식물을 주로 먹거나 성장 발육이 필요로 하는 양 이하의 음식물을 장기 간 먹을 때,
-
체질에 맞지 않는 음식물이나 인공영양을 먹을 때,
-
권장한 대로 인공영양을 먹지 않을 때,
-
권장한 칼로리 양보다 훨씬 적은 칼로리 양의 인공영양을 먹을 때,
-
단백질이 조금도 들어 있지 않은 음식물을 오랫동안 먹을 때,
-
비타민이 충분히 들어 있지 않은 음식물을 먹을 때,
-
먹든 말든 자유자제로 음식물을 먹도록 방치해서 육아할 때,
-
균형 잡힌 음식물을 먹든지 안 먹든지 상관치 않고 육아할 때,
-
비타민 A와 비타민 D를 과량으로 섭취할 때
-
성장 호르몬 저하증, 갑상선 기능 저하증, 갑상선 기능 항진증, 난소 기능 저하증, 고환 기능 저하증, 부신피질 기능 저하증, 당뇨병 등의 내분비선 질환이 있는 아이들
-
심한 선천성 심장 질환이나 후천성 심장 질환이 있는 아이들
-
심한 기관지 천식, 기관지 확장 증, 또는 그 외 심한 호흡기 질환이 있는 아이들
-
연골 이상이나 경골 이상이 있거나 구루병이 있는 아이들
-
우유 단백질 알레르기나 유당 불내증이 있는 아이들,
-
염증성 장염으로 장기간 설사하는 아이들,
-
람불편모충증 등 기생충증이 있는 아이들,
-
보리·밀가루·호밀·귀리의 음식물 속에 든 글루텐 단백질로 생기는 셀이악 병(글루텐 장염)이 있는 아이들
-
그 외 다른 종류의 음식물 불내증이나 음식물 알레르기로 장기간 설사하는 아이들
-
만성 빈혈이 있거나 그 밖의 다른 혈액 질환이 있는 아이들
-
폐, 신장, 골, 그 외 다른 장기에 만성 감염병이 있어 영양실조가 된 아이들
-
뇌수종(수두증)·뇌종양·뇌출혈 등 중추신경계 질환이 있는 아이들
-
만성 요로 감염이나 신장 질환이나 신장 비뇨계 질환이 있는 아이들
-
급성 간염 또는 만성 간염 등의 간 질환이 있는 아이들
-
병적 위 식도 역류병으로
-
후부 요도 판막증으로
-
그 외
2. 성장 중지증의 내적 원인
-
타고날 때부터 체질이 작은 부모로부터 태어난 아이들은 정상적으로 늦은 성장속도로 작게 자라는 것이 보통이다.
-
다운 증후군, 터너 증후군 등 염색체 이상이 있는 아이들
성장 중지증(성장 부전, 성장 실패, 성장 장애)의 진단 치료
-
앞서 설명한 것과 같이 어떤 아이의 체중이 적절한 성장 속도로 잘 자라지 않는 원인은 많다.
-
어떤 때는 확실한 원인을 찾아낼 수 없다.
-
아이의 체중이 적절히 늘지 않고 성장 중지증이 있다고 의심이 되면 과거 병력, 현재 병력, 가족 병력, 음식물 섭취 패턴 등 자세한 정보를 얻고 자세히 진찰하고 필요에 따라 대소변검사·피검사·가슴 X-선 검사 등을 한다.
-
건강 검진이 정상이고 대체적으로 건강하고 성장 중지증의 원인을 확실히 모를 때는 일정한 기간을 두고 추적 재검진을 하고
-
추적 임상검사 등을 반복하기도 한다.
-
아이의 체중과 신장이 성장차트의 체중 백분위선과 신장 백분위선을 따라 적절히 계속 증가되는지 관찰하면서 원인을 찾아낼 때도 있다.
-
친 부모 형제자매들이 타고난 체질에 따라 성장할 때처럼 잘 먹고 잘 놀고 자라면서 신체 전체가 균형 잡히고 체구가 작은 아이는 특별한 검사를 받을 필요도 없고 아무 치료를 받을 필요도 없다.
-
체중이 비정상적으로 작고 잘 자라지 않는 성장 중지증이 현저하게 있을 때는 필요에 따라 병원에 입원하여 진찰 진단, 임상 검사, 관찰하면서 치료해야 할 때도 있다.
-
병원에 입원하고 있는 동안 간호사와 의사가 그 아이의 하루하루 일거일동을 관찰하고, 음식물의 섭취량, 부모–자녀 상호관계를 살펴보고, 그 아이와 간호사 간의 상호작용, 또는 의사와의 상호작용, 수면패턴 등을 통괄적으로 관찰하고 여러 번 반복적으로 진찰하고 필요에 따라 여러 가지 임상 검사를 반복해서 그 원인을 찾아내는 경우도 있다.
-
성장 중지증의 원인을 찾으면 그 원인에 따라 치료한다.
Failure to thrive (growth failure/growth failure/growth disorder) 성장 중지증(성장 부전/성장 실패/성장 장애)
Figure 5-6. An example of a growth chart of Boknam-i growing along the 50th percentile line from 0-36 months of age (left) An example of a growth chart of Boknam-i growing along the 50th percentile line during the age of 2-18 (right) Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 5-5. An example of a growth chart for girls in newborns and infancy growing along the 50th percentile from 0 to 36 months of age (left) Examples of growth charts for infants, school-age, and puberty girls growing along the 50th percentile during the age of 2-18 years old (right) Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Bringing young infants and toddlers to the Pediatrics Department and said, “My child eats well, eats an egg every day, drinks a cup of milk, eats enough meat, eats vitamins every day, and I don’t know why it’s not so big!” Sometimes parents make appeals and ask for detailed examination of the reason.
• Sometimes parents ask, “He’s always bleeding, pale, and energetic. Ask him to see if he has anemia or parasites.”
• If the child’s height and weight are measured and examined in detail from head to toe, CBC blood test, small stool test, and other appropriate tests are performed. There is no anemia, blood, urine, and stool tests are all normal, and the stool is parasites. There are no eggs or adults, and their children are often evaluated as healthy children who grow up properly and properly.
• At that time, the parent draws the child’s weight and height on a growth chart, showing the weight percentile and height percentile, while the child’s weight follows the child’s weight percentile, and the height grows normally according to the child’s height percentile. When you show parents that they are growing well at a fast pace and explain their children’s growth well, they are relieved of understanding that their children are growing normally. www.drleepediatrics.com-Vol. 14 Pediatric and adolescent Endocrine, genetics, chromosomes, metabolism, see rare diseases.
• In addition, explaining that the child will continue to grow at about the same growth rate as his or her previous growth rate, and the estimated weight and height at the age of 18 will show that the parent feels more relieved.
• Rarely, there are rare cases in which the food consumed by a young infant during that period does not fit the child’s constitution and does not get enough nutrients and calories to gain normal weight and overall growth and development is delayed. However, due to regular health check-ups, this phenomenon is very rare these days.
• Some diseases may prevent you from gaining adequate weight for your age. Sometimes growth can be abnormally delayed or stopped.
• If a child’s weight does not increase well or seems to have stopped growing according to the child’s innate growth rate, undergo a physical examination to find the cause, and conduct an appropriate clinical examination with the subject such as blood, urine, and stool. Sometimes it is necessary to determine the cause.
• Parents believed that the child was growing properly until the child was brought to the Department of Pediatrics and adolescents to conduct regular health check-ups on a regular basis. However, the child received regular medical check-ups at the Department of Child and Adolescents and the child grew and developed appropriately. Sometimes the first time you are diagnosed that it doesn’t work.
• Sometimes the growth rate of height and weight is unusually much slower than children of their age for some reason, but some children are congenital and very small because they do not grow properly. So you can be diagnosed as if you have dystrophy.
• In summary, when a child’s weight or height growth rate is significantly slower than that of children of the same age as the child’s gender, it is defined as abortion, growth failure, growth failure, or failure to thrive www.drleepediatrics.com-Vol. 14 Pediatric Endocrine, Genetics, Chromosomes, Metabolism, Rare Diseases-Refer to Short Children).
Causes of abortion
1. External causes of Failure to thrive
• When you are poor and cannot get enough food,
• When eating mainly foods with little nutritional value or eating foods less than the amount required for growth and development for a long period of time,
• When eating food or artificial nutrition that does not fit your constitution, • When not eating artificial nutrition as recommended,
• When eating artificial nutrients with calories much less than the recommended calorie amount,
• When eating foods that do not contain any protein for a long time,
• When eating foods that do not contain enough vitamins,
• When raising children by neglecting to eat food freely, whether they eat or not, • When raising children regardless of whether they eat a balanced diet or not,
• When you take too much vitamin A and vitamin D
• Children with endocrine diseases such as hypogonadism, hypothyroidism, hyperthyroidism, ovarian hypofunction, hypotesticular function, hypoadrenocortical function, diabetes, etc.
• Children with severe congenital or acquired heart disease
• Children with severe bronchial asthma, bronchiectasis, or other severe respiratory problems
• Children with cartilage abnormalities, tibia abnormalities, or rickets
• Children with milk protein allergy or lactose intolerance,
• Children with prolonged diarrhea due to inflammatory enteritis,
• Children with parasitic diseases such as Lambite caterpillars,
• Children with celiac disease (gluten enteritis) caused by gluten protein in foods of barley, wheat flour, rye, and oats
• Children with long-term diarrhea due to other types of food intolerance or food allergies
• Children with chronic anemia or other blood disorders
• Children who are malnourished due to chronic infectious diseases in the lungs, kidneys, bones, and other organs
• Children with central nervous system diseases such as hydrocephalus (hydrocephalus), brain tumor, cerebral hemorrhage
• Children with chronic urinary tract infections or kidney disease or kidney and urinary system disease
• Children with liver disease, such as acute hepatitis or chronic hepatitis
• pathological gastroesophageal reflux disease
• With posterior urethral valve disease
• etc
2. Internal causes of Failure to thrive
• It is common for children born from parents with small constitutions from birth to grow small at a normal slow growth rate.
• Children with chromosomal abnormalities such as Down syndrome and Turner syndrome
Diagnosis, treatment of Failure to thrive(growth failure, growth disorder)
• As explained above, there are many reasons why a child’s weight does not grow well at an appropriate growth rate.
• Sometimes it is impossible to find a definite cause.
• If a child’s weight is not gaining adequately and is suspected of having dysplasia, obtain detailed information such as past medical history, current medical history, family medical history, food intake patterns, etc., and examine them in detail, feces, blood, and chest X-rays as necessary. Etc.
• When the medical examination is normal and generally healthy, and the cause of the dystrophy is unclear, follow-up re-examination is performed over a period of time.
• Follow-up clinical tests may be repeated.
• In some cases, the cause is identified by observing whether the child’s weight and height continue to increase properly along the weight percentile and height percentile on the growth chart.
• Parents, siblings, and siblings eat well, play well, and grow up as they grow up according to their natural constitution, so that the whole body is in balance and small children do not need any special examination or treatment.
• When the weight is abnormally small and there is remarkable abortion, which is not growing well, you may need to be admitted to a hospital and treated with medical examination, clinical examination, and observation as needed.
• While in the hospital, nurses and doctors monitor the child’s daily routines, look at food intake, parent-child interactions, interactions between the child and the nurse, or interactions with the doctor, and sleep. In some cases, patterns, etc., are observed comprehensively, and the cause is repeatedly examined several times, and various clinical tests are repeated as needed.
• If you find the cause of dystrophy, treat it according to the cause.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drle epediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
-
[부모도 반의사가 되어야 한다– 소아가정간호백과]-제 14장 소아 내분비계 염색체, 대사 질환 내분비선 성장차트 0~36개월 남아성장차트, 2~18세 남아성장차트, 0~36개월 여아 상장차트, 2~18세 여아성장차트
-
The pregnancy Bible. By Joan stone,MD. Keith Eddleman,MD
-
Preparation for Birth. Berverly Savage and Dianna Smith
-
임신에서 신생아 돌보기까지. 장중화, 이상원
-
Breastfeeding. by Ruth Lawrence and Robert Lawrence
-
Groowth anfd developement of children by G. H. Lowrey
-
Nelson Textbook of Pediatrics 14th ed.Beherman,
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition Growth and Development of children. George H. Lowerey 8th Ed
- Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey grant, and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
- The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
- Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Manual of Emergency Care
- 응급환자관리 정담미디어
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- Neonatal Resuscitation American heart Association
- Neonatology Jeffrey J.Pomerance, C. Joan Richardson
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
- Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
- Preparation for Birth. Beverly Savage and Dianna Smith
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
- Red book 29th edition 2012
- Nelson Text Book of Pediatrics 19th Edition
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- 소아과학 대한교과서
- 제1권 소아청소년 응급의료 참조문헌과 출처
- Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”