선천성 거대결장 Congenital megacolon

그림 142. 선천성 거대결장.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
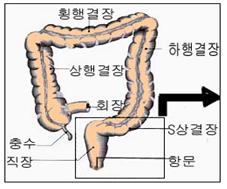
그림 141. 정상 대장.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
선천성 거대결장의 원인
-
항문과 S상 결장 사이에 있는 대장 부분을 직장이라 하고 그 직장의 최상부는 S상 결장으로 연결되고 직장의 최 하부는 항문으로 연결된다.(그림 141참조)
-
S상 결장, 직장, 그 외 대장관(상행결장+횡행결장+하행결장)의 장벽에 부교감신경과 교감신경이 정상적으로 분포되어 있다.
-
교감신경과 부교감신경은 직장, S상 결장, 하행결장, 횡행결장, 상행결장 등 위장관 연동운동 을 조절하는 기능을 가지고 있다.
-
먹은 소대장관 속 소화된 음식물은 소장관 속, 대장관 속에서 연동운동으로 S상 결장관 속 , 직장관 속을 거쳐 항문 속 쪽으로 내려가는 것이 정상이다.
-
항문, 직장관 장벽 또는 S상 결장관 장벽의 일부분이나 전체에 있는 부교감신경절이 선천적으로 없을 수 있다. 부교감신경절이 선천적으로 없는 S상 결장관의 벽이나 직장관 벽에 연동운동 작용이 정상적으로 생기지 않게 된다. 이 때 S상 결장관 속이나 직장관 속의 일부분이 부분적으로 막히거나 완전히 막힐 수 있다.
-
먹은 음식물의 대부분은 위 소장관 속에서 소화되어 영양분이 핏속으로 흡수되고 소화되지 않은 잔여물이 대변이 된다. 그 잔여물이 부교감신경절이 정상적으로 분포되어 있는 직장관 부분이나 S상 결장관의 부분까지 정상적 연동운동 작용으로 내려올 수 있으나 부교감신경절이 정상적으로 분포되어 있지 않은 S상 결장관이나 직장관의 부분 이하 부분으로는 더 이상 내려갈 수 없다.
-
그에 따라 변비증이 심하게 또는 경하게 생길 수 있다. 때로는 S장 결장관이나 직장관 장폐쇄증도 생길 수 있다.
-
이런 병을 선천성 거대결장, 또는 히르시스프룽병(Hirschsprung’s disease)이라고 한다.
선천성 거대결장의 증상 징후
-
부교감신경 절이 선천적으로 어느 정도로 없느냐, 부교감신경 절이 없는 S상 결장관이나 직장관 부분의 길이, 부교감신경 절이 S상 결장관이나 직장관의 어느 부분에 없는지, 나이에 따라 증상 징후가 다르다.
-
먹은 음식물의 일부는 위장관 속에서 소화된 후 위장관 벽 점막층을 통해 피로 흡수되고 소화되지 않은 잔여물은 대변으로 나오는 것이 정상이다.
-
이 병이 있을 때는 대변이 부교감신경 절이 없는 S상 결장관 속이나 직장관 속까지 연동운동 작용으로 도착한 후 더 이상 항문 속 쪽으로 내려갈 수가 없다.
-
이 때 부교감신경 절이 없는 S상 결장관 속이나 직장관 속의 부분의 바로 위에 있는 S상 결장관 부분 속이나 직장관 속에 연동운동 작용으로 내려온 소화되지 않은 잔여물–대변이 가득 차있고 그 부위의 S상 결장관이나 직장관이 비정상적으로 확장될 수 있다.
-
부교감신경 절이 없는 S상 결장관 속이나 직장관 속의 바로 아래에 있는 S상 결장관 속이나 직장관 속에는 대변이 조금 차 있거나 아주 없을 수 있다.
-
부교감신경 절이 없는 S상 결장관 속이나 직장관의 속의 바로 아래에 있는 S상 결장관의 나머지 부분이나 직장관의 크기는 정상 이하로 작다(그림 142 참조).
-
이 병이 있으면 대변을 전혀 보지 못하거나 아주 조금 보든지 또는 심한 변비증에 걸리게 된다.
-
이 병이 있는 어떤 신생아는 태변을 생후 2~3일 이후에 조금 볼 수도 있고, 그 후 1 주 동안 1회 정도 대변을 보기도 한다.
-
대변을 볼 때 힘을 주고 울기도 하고 방귀를 많이 끼기도 한다. 체중이 잘 늘지 않고 아래 배에서 대변 덩어리가 만져질 수도 있고 심한 변비증이 있을 수 있다.
-
이 선천성 위장관 기형은 흔하지는 않지만 신생아나 영유아에게 변비증이 심할 때는 한 번 정도 이 병이 있나 의심해 볼 수 있는 병이다.
선천성 거대결장의 진단
-
병력·증상 징후·진찰소견 등을 종합해 이 병이 의심되면 S상 결장관·직장관·항문 바륨액 X-선 사진 검사, 직장관과 S상 결장관 내시경검사, S상 결장관 장벽이나 직장관 장벽 부교감신경절 생체 조직검사 등으로 진단할 수 있다.
선천성 거대결장의 치료
- 부교감신경 절이 없는 결장관이나 직장관의 부분을 절제하고 정상 부분을 서로 연결하는 수술치료를 한다.
Congenital megacolon 선천성 거대결장
Figure 142. Congenital large colon. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 141. Normal large intestine. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Causes of congenital megacolon
• The part of the large intestine between the anus and the sigmoid colon is called the rectum, and the uppermost part of the rectum is connected to the sigmoid colon and the lowermost part of the rectum is connected to the anus (see Figure 141).
• Parasympathetic nerves and sympathetic nerves are normally distributed in the sigmoid colon, rectum, and other barriers of the colon (ascending colon + transverse colon + descending colon).
• The sympathetic and parasympathetic nerves have the function of controlling gastrointestinal peristalsis such as rectum, sigmoid colon, descending colon, transverse colon, and ascending colon.
• It is normal for the digested food in the small intestine to go down into the anus through the sigmoid colon and rectal duct through peristalsis in the small intestine and the colon.
• Parasympathetic ganglions in part or all of the anus, rectal barrier, or sigmoid barrier may be congenital absent. Peristalsis does not normally occur on the wall of the sigmoid duct or the rectal duct wall, where the parasympathetic ganglion is not congenital. In this case, the sigmoid colon or part of the rectal canal may be partially or completely blocked.
• Most of the food eaten is digested in the stomach and small intestine, nutrients are absorbed into the blood, and undigested residues become feces. The residue may come down to the part of the rectal duct where the parasympathetic ganglia are normally distributed or the part of the S-phase colon duct by normal peristalsis, but the part below the part of the S-phase or rectal duct where the parasympathetic ganglion is not normally distributed. Can no longer go down.
• This can lead to severe or mild constipation. Sometimes sigmoid colon or rectal tract obstruction can occur.
• This disease is called congenital megacolon, or Hirschsprung’s disease.
Signs of the symptoms of a congenital megacolon
• Symptoms differ according to age, to what extent the parasympathetic ganglion is present, the length of the sigmoid or rectal duct without a parasympathetic ganglion, whether the parasympathetic ganglion is located in the sigmoid or rectal duct.
• It is normal for some of the food eaten to be digested in the gastrointestinal tract and then absorbed by the blood through the mucous membrane of the gastrointestinal tract, and the undigested residues come out in the stool.
• With this disease, the stool reaches into the sigmoid colon without parasympathetic ganglion or into the rectal canal through peristalsis, and then can no longer descend into the anus.
• At this time, undigested residues descended from peristalsis in the sigmoid tract or rectal duct directly above the sigmoid duct or rectal duct without parasympathetic ganglia-the stool is full The upper colon or rectal canal may be abnormally dilated.
• There may be little or no stool in the sigmoid tract without a parasympathetic ganglion or in the sigmoid tract or rectal duct directly below the rectal duct.
• The rest of the sigmoid duct without a parasympathetic ganglion or the rest of the sigmoid tract or the rectal duct located just below the inside of the rectal duct is smaller than normal (see Figure 142).
• With this disease, you may not see any stool, see very little, or cause severe constipation.
• Some newborns with this disease may have a slight meconium 2 to 3 days after birth, and then stool once a week.
• When I stool, I feel empowered, cry, and fart a lot. You may not gain weight well, you may feel a lump of stool in your lower stomach, or you may have severe constipation.
• This congenital gastrointestinal deformity is not common, but when constipation is severe in newborns or infants, it is possible to suspect that they have the disease.
Diagnosis of congenital megacolon
• Comprehensive history, symptoms, medical findings, etc. If you suspect this disease, sigmoid colon, rectal duct, anal barium liquid X-ray examination, rectal and sigmoid duct endoscopy, sigmoid duct barrier or It can be diagnosed by biopsy of the rectal barrier parasympathetic ganglion.
Treatment of congenital megacolon
• Excision of the part of the colon or rectal canal without the parasympathetic ganglion, and surgical treatment that connects the normal parts to each other.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey grant, and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
- The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
- Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Manual of Emergency Care
- 응급환자관리 정담미디어
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- Neonatal Resuscitation American heart Association
- Neonatology Jeffrey J.Pomerance, C. Joan Richardson
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
- Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
- Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- 소아과학 대한교과서
- 제1권 소아청소년 응급의료 참조문헌과 출처
- Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”