서혜부 탈장(서혜 헤르니아/서혜 탈장) Inguinal hernia
서혜부 탈장의 개요
- 횡격막 헤르니아(Diaphragmatic hernia/가로막이탈), 원반 탈출증(Herniated disc), 추간판 탈출증, 궁둥구멍 탈장(Sciatic hernia), 좌골공 탈장(Scrotal hernia), 음낭 헤르니아(Sliding hiatal hernia), 양측성 서혜부 탈장 등 여러 종류의 탈장 및 헤르니아가 신체 여러 부위에 생길 수 있다.
- 직접형 서혜부 탈장(Direct inguinal hernia), 간접형 서혜 탈장(Indirect inguinal hernia) 두 가지가 있고 일측성 서혜부 탈장 또는 양측성 서혜부 탈장이 있다. 또 선천성 완전 서혜부 음낭 헤르니아가 있다.
- 임신 6~7개월까지 태아의 양쪽 고환은 복강 내에 있는 것이 보통이다.
- 그 후 양쪽 고환이 복강 내에서 서혜관 속을 통과해 음낭 속으로 이동된다.
- 그 후부터 고환이 음낭 속에 계속 머물러 있는 것이 정상이다.
- 복강 속에 있던 고환이 서혜관(Inguinal canal)을 통과한 후 음낭 속으로 내려온 후 서혜관이 완전히 막히는 것이 정상이다.
- 때로는 한쪽 서혜관이나 양쪽 서혜관이 완전히 막히지 않을 수 있다.
- 이 때 복강 내 복막의 일부나, 여성인 경우, 난소, 또는 장관의 일부분 등이 막히지 않은 서혜관 속을 통과해 복벽 밖에 있는 대음순 속으로 나올 수 있고 남성인 경우, 복강 내 복막의 일부, 장관의 일부가 서혜관 속을 통과하여 음낭 속, 또는 음낭 바로 위에 있는 서혜관 속 등으로 빠져 나올 수 있다.
- 이것을 간접형 서혜부 탈장이라고 한다.
- 간접형 서혜부 탈장은 여아들에게보다 남아들에게 더 잘 생긴다. 다음은 간접형 서혜부 탈장에 대해서 주로 설명한다.
서혜부 탈장(서혜 헤르니아/서혜탈장)의 원인
- 원인은 아직도 확실히 모른다.
- 서혜부 탈장의 발생률은 만삭 신생아들 중 약 1~5%이고 비교적 큰 미숙 신생아들 중 9~10%이고 아주 더 작은 미숙 신생아들에게는 그 보다 더 많이 발생한다.
- 남아와 여아의 서혜부 탈장의 발생률의 비율은 5:1이다.
- 60%는 우측에 생기고 10%는 양측성이다(출처; Contemporary pediatrics, December 2008. p.516).
- 고환이 음낭 속에 없이 태어난 아이, 그밖에 다른 종류의 선천성 기형을 갖고 태어난 아이들에게 간접형 서혜부 탈장이 더 잘 생길 수 있다.

사진 234. 유아 양쪽 서혜부에 있는 간접형 서혜부 탈장
탈장으로 인해 양쪽 서혜부가 볼록해 보인다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
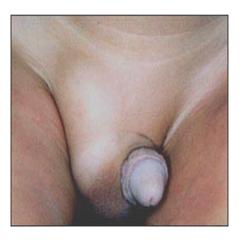
사진 235. 잠시 후 왼쪽 간접형 서혜부 탈장 내용물이 복강 내로 들어가서 왼쪽 서혜부는 정상적으로 보이나 오른쪽 서혜부 속에 그대로 있는 서혜부 탈장으로 인해 볼록하게 보인다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
서혜부 탈장(서혜 헤르니아, 서혜탈장)의 증상 징후
- 증상 징후는 다양하다.
- 서혜부 탈장이 출생 시 나타날 수도 있고 첫 돌이 오기 전 영아기에 나타날 수도 있다.
- 복강 내 장관의 일부분, 복막의 일부분, 난소 등이 서혜부 속으로, 서혜부 바로 아래부위 속으로, 음낭 속 또는 대음순 속으로 나와 간접형 서혜부 탈장이 남녀의 성에 따라 각각 생길 수 있다. 이 때 탈장으로 서혜부가 불쑥 나온 것을 육안으로 볼 수 있다(사진 234, 235 참조).
- 탈장 속에 들어 있는 장관의 일부분이나 복막의 일부분으로 불쑥 나온 탈장을 손으로 만져볼 수 있다.
- 서혜부 탈장 속에 나와 있는 장관의 일부분이나 복막의 일부분의 크기에 따라 서혜부 탈장의 크기도 다르다.
- 서혜부 탈장은 밤알만 한 것도 있고 달걀만 한 것도 있다.
- 서혜부 탈장이 있을 때 장관의 일부분이나 복막의 일부분이 복강 내에서 서혜관 속을 통과해 서혜부 속이나 대음순 속, 음낭 속, 음낭 바로 윗부분 서혜관 속으로 빠져 나온 후 아무 증상이 없이 그대로 얼마동안 있다가 탈장된 장관의 일부나 복막의 일부가 복강 내로 다시 들어가 얼마 동안 그 상태로 있을 수 있다(사진 235 참조).
- 이와 같이 복강 내로 들어갔던 탈장 내용물이 복강 밖으로 다시 나왔다가 복강 내로 다시 들어갔다 나왔다 할 수 있다.
- 다시 설명하면, 서혜부 탈장 내용물이 서혜관 속을 통과 한 다음 복벽 서혜관을 통과해서 복강 내로, 다시 들어갔다가 복강 외로 다시 나오는 식으로 들락날락한다.
- 특히 서혜부 탈장이 있는 영유아가 울 때나 대변을 보기 위해 배에 힘을 많이 주어 복강 내 압을 증가될 때, 대변을 보기 위해서 복강 내로 힘을 많이 줄 때, 또는 기침할 때 복강 내압이 증가될 때 복강 내로 들어가 있던 서혜부 탈장 내용물이 복강 속 밖에 있는 서혜관 속으로 다시 나올 수도 있고, 또 이미 복강 내에서 서혜관 속으로나 음낭 속으로 나와 있던 탈장 내용물이 더 커질 수 있고 서혜부나 음낭이 볼록하게 커지는 것이 보통이다.
- 서혜부 탈장이 있는 아이가 가만히 누워 휴식을 취하거나, 잠잘 때에는 서혜부 탈장 속에 있던 탈장 내용물이 복강 내로 다시 들어가 있을 수 있다.
- 육체적으로 매우 활동적인 사춘기 아이에게 있는 서혜부 탈장의 내용물이 서혜관 속으로 나온 후 그 탈장 내용물이 더 이상 복강 내로 들어가지 않고 복강 속 바깥 서혜관 속에 계속 머물러 있는 경우도 있다.
- 서혜부 탈장이 있을 때 서혜부 속에 나온 장관의 일부나 복막의 일부 또는 난소 등이 서혜관 속을 통과해서 복강 내로 들어갔다 나왔다 하는 것이 보통이지만, 복강 속 바깥에 있는 서혜관 속으로 일단 나왔던 탈장 내용물이 또다시 복강 내로 더 이상 저절로 들어가지 못할 때가 있다.
- 손가락으로 그 탈장 내용물을 복강 내로 밀어 넣어도 탈장 내용물이 복강 내로 더 이상 들어가지 않을 때도 있다.
- 이런 경우를 헤르니아가 감돈됐다고 한다. 이 병을 헤르니아 감돈이라고 한다.
- 서혜부 탈장이 감돈 되었을 때에는 서혜관 속으로 나온 복막의 일부분이나 장관의 일부분 등의 탈장 내용물에 있는 혈액 순환이 정상적으로 되지 않기 때문에 탈장 내용물이 괴사되고 손상될 수 있다.
- 이 때 장폐색증 등이 생길 수 있고 그에 따른 증상 징후가 생길 수 있다. 그리고 심한 복통과 구토가 생길 수 있다.
- 신생아에게 있는 서혜부 탈장은 더 쉽게 감돈 될 수 있다. 또 서혜부 탈장이 감돈 되었을 때에는 응급 수술치료를 받지 않으면 생명에도 위험할 수 있다.
서혜부 탈장(서혜 헤르니아/서혜 탈장)의 진단
- 병력, 증상 징후, 진찰소견 등을 종합하여 이 병을 진단한다.
- 서혜부 탈장 내용물은 서혜관 속을 통해 복강 내로 들어갔다 복강 속 밖으로 나왔다 하는 것이 보통이다.
- 탈장 내용물이 복강 내에 들어가 있는 동안에 의사가 진찰을 할 때는 서혜부 탈장이 있는지 없는지 그냥 보고서 확실히 진단 할 수 없다.
- 그러나 진찰을 할 때 배에 힘을 많이 주면 복강 내압이 높아져서 복강 내 탈장 내용물이 서혜관 속으로 나올 수 있다.
- 이 때, 서혜부 탈장을 보고 쉽게 진단할 수 있다.
서혜부 탈장(서혜 헤르니아/서혜탈장)의 치료
- 서혜부 탈장 내용물이 복강 내로 쉽게 들어갔다 나왔다 하고 아무 증상 징후가 없어도 적절한 시기에 선택적 수술 치료를 한다.
- 특히 신생아들이나 영유아들의 서혜부 탈장증은 가능한 한 속히 선택적 수술 치료를 해 주는 것이 좋다. 서혜부 탈장이 감돈되면 응급 수술 치료를 해야 하기 때문이다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제6권 신생아 성장 발육 양호 질환 -신생아 외음부 신생아의 식도, 위, 소장, 대장 등의 폐쇄증 참조
Inguinal hernia 서혜부 탈장(서혜 헤르니아/서혜탈장)
Overview of inguinal hernia
‘• Diaphragmatic hernia, Herniated disc, intervertebral disc herniation, Sciatic hernia, Scrotal hernia, Sliding hiatal hernia, bilateral inguinal hernia, etc. Different types of hernias and hernias can occur in different parts of the body.
• There are two types: direct inguinal hernia and indirect inguinal hernia, and unilateral inguinal hernia or bilateral inguinal hernia. There is also a congenital complete inguinal scrotal hernia.
• By the 6th to 7th month of pregnancy, both testicles of the fetus are usually in the abdominal cavity.
• After that, both testicles are moved from the abdominal cavity through the inguinal tract into the scrotum.
• From then on, it is normal for the testicles to remain in the scrotum.
• It is normal for the inguinal canal to be completely blocked after the testicle in the abdominal cavity passes through the inguinal canal and descends into the scrotum.
• Sometimes one groin or both groin canals may not be completely blocked.
• At this time, a part of the peritoneum in the abdominal cavity, in the case of a woman, the ovary, or part of the intestine, can pass through the unblocked inguinal tract and come out into the labia majora outside the abdominal wall. In the case of a male, part of the peritoneum in the abdominal cavity, the intestinal tract Some may pass through the groin canal and exit into the scrotum, or into the groin canal just above the scrotum.
• This is called an indirect inguinal hernia.
• Indirect inguinal hernia is more common in boys than in girls.
The following mainly describes indirect groin hernia.
Causes of inguinal hernia (inguinal hernia/inguinal hernia)
• The cause is still unknown.
• The incidence of inguinal hernias is about 1-5% of full-term newborns, 9-10% of relatively large premature newborns, and even more in very small premature newborns. • The ratio of incidence of inguinal hernia in boys and girls is 5:1.
• 60% occurs on the right side and 10% is bilateral (source; Contemporary pediatrics, December 2008. p.516).
• Indirect groin hernias are more likely to develop in children born with no testicles in the scrotum, as well as children born with other types of congenital anomalies.
Photo 234. Indirect groin hernia in both groin areas of infants. Both groin areas appear convex due to hernia. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Photo 235. After a while, the contents of the left indirect groin hernia enters the abdominal cavity, and the left groin is seen normally, but it looks convex due to the inguinal hernia remaining in the right groin. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Symptoms,signs of a groin hernia (inguinal hernia, inguinal hernia)
• Symptom signs vary.
• A groin hernia may appear at birth or may appear in infancy before the first stone.
• A part of the intestinal tract, part of the peritoneum, and ovaries in the abdominal cavity may come into the groin, just below the groin, into the scrotum or into the labia majora, and an indirect groin hernia may occur depending on the sex of the sex of the male and female. At this time, it is possible to see with the naked eye that the groin protrusion was protruded due to a hernia (see photos 234 and 235).
• Part of the intestinal tract in the hernia or a hernia that has protruded as part of the peritoneum can be touched with your hand.
• The size of the inguinal hernia is also different depending on the size of the part of the intestinal tract or the part of the peritoneum in the groin hernia.
• Some inguinal hernias are chestnut-sized and some are only eggs.
• When there is a groin hernia, part of the intestine or peritoneum passes through the groin duct from the abdominal cavity and exits into the groin, labia majora, scrotum, and the groin canal just above the scrotum. Part of the intestinal tract or part of the peritoneum may re-enter the abdominal cavity and remain there for some time (see photo 235). • In this way, the contents of the hernia that entered the abdominal cavity may come out of the abdominal cavity and then enter and exit the abdominal cavity again.
• In other words, the contents of the inguinal hernia pass through the groin tube, then through the abdominal wall, into the abdominal cavity, then into and out of the abdominal cavity, in and out of the abdominal cavity.
• When infants and toddlers with a groin hernia cry or when pressure is increased in the abdominal cavity by applying a lot of pressure to the stomach to see a bowel movement, when a lot of pressure is applied to the abdominal cavity to see a stool, or when the intra-abdominal pressure increases when coughing. The contents of the inguinal hernia that had entered the abdominal cavity may come out again into the groin duct outside the abdominal cavity, and the contents of the hernia that were already in the abdominal cavity into the groin duct or into the scrotum may become larger, and the groin or scrotum is usually convexly enlarged.
• When a child with a groin hernia lies still and rests, or when sleeping, the contents of the hernia from the groin hernia may re-enter the abdominal cavity.
• In some cases, the contents of a groin hernia in a physically active adolescent child come out into the groin duct, and the contents of the hernia no longer enter the abdominal cavity and remain in the outer groin duct in the abdominal cavity.
• When there is a groin hernia, it is common to say that part of the intestinal tract, part of the peritoneum, or ovary from the groin is passed through the groin and enters and exits into the abdominal cavity. There are times when you can no longer go into yourself on your own.
• Sometimes, the hernia contents no longer enter the abdominal cavity when the contents of the hernia are pushed into the abdominal cavity with a finger.
• In this case, it is said that hernia was imprisoned. This disease is called Hernia Gamdon.
• When the inguinal hernia is confined, blood circulation in the hernia contents such as a part of the peritoneum or a part of the intestine that has come out into the inguinal tract is not normal, so the hernia contents may be necrotic and damaged.
• At this time, intestinal obstruction, etc. may occur, and symptoms may occur. It can also cause severe abdominal pain and vomiting.
• In newborns, inguinal hernias can be more easily closed. In addition, when an inguinal hernia is confined, it can be dangerous to life if you do not receive emergency surgical treatment.
Diagnosis of inguinal hernia (inguinal hernia/inguinal hernia)
• Diagnose this disease by synthesizing the medical history, symptoms, and examination findings.
• It is common for the contents of the inguinal hernia to enter the abdominal cavity through the groin tube and come out of the abdominal cavity.
• When the doctor examines the hernia while the contents are in the abdominal cavity, it is not possible to diagnose with certainty just by looking for the presence or absence of a groin hernia.
• However, if a lot of pressure is applied to the stomach during a medical examination, the intra-abdominal pressure may increase and the contents of the hernia in the abdominal cavity may come out into the inguinal tract.
• At this time, it can be easily diagnosed by looking at the inguinal hernia.
Treatment of inguinal hernia (inguinal hernia/inguinal hernia)
• Even if the contents of the inguinal hernia easily enters and exits the abdominal cavity, and there are no signs of symptoms, selective surgical treatment is performed at the appropriate time
. • In particular, it is advisable to provide selective surgical treatment for inguinal hernia in newborns or infants as soon as possible. This is because if the inguinal hernia is confined, emergency surgical treatment is required.www.drleepediatrics.com-Volume 6 Neonatal growth and development disease-Newborn vulva Refer to atresia of the esophagus, stomach, small intestine, and colon
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com 제7권 소아청소년 감염병
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, harvey grant, and robert murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”