사춘기 아이들의 우울증 Depression in adolescents(Adolescent depression /Teen depression)
사춘기 아이들의 우울증의 개요
- 우울증은 위중한 정신 질환 중 하나이고 남녀노소 빈부를 가르지 앓고 사회각계 각층 누구에게 생길 수 있다.
- 소아청소년기에 심한 우울증을 한번이라도 앓으면 그 후 5년 이내 우울증이 재발될 가능성이 많다.
- 사춘기 이전 영유아들, 학령기 아이들이나 사춘기 아이들에게 양극성 정신장애(Bipolar disorder)가 1994년 이래 40배나 증가됐다(출처; Dr. Mark Olson, The Journal of archives of general psychiatry 2007).
- 소아청소년들 10명 중 1명이 우울증에 걸릴 수 있다.
- 사춘기 아이들의 4~18%이 우울증에 걸린다.
- 심각한 정신병을 앓고 있는 미 사춘기 아이들 중 30%만 적절한 치료를 받고 있다.
- 심각한 정신병을 가진 성인들의 50%는 14세 경부터 정신병이 시작됐다고 한다(출처; Journal watch pediatrics and adolescent medicine, August 2008. p.769).
- 우울증의 주증은
-
- 느낌 장애와
- 행동 장애이다.
- 정신건강 상태가 전반적으로 나빠질 수 있다.
- 우울증에 걸린 대부분의 아이들은 적절한 치료를 곧 받지만 일부는 자신이 우울증에 걸려 있는 줄도 모르고 있다. 그들의 부모들도 자녀에게 우울증이 있는지도 모르고 있다. 그 때문에 우울증이 있는 아이들이 적절한 우울증 치료를 받지 않는 경우도 흔하다.
- 적절히 치료 받으라고 권장해도 치료를 적절히 받지 않는 경우도 흔하다.
- 사춘기 아이들의 우울증은 자살의 주원인이 된다.
- 자살은 15~24세 후기 사춘기 아이들과 젊은이들의 사망의 원인의 3번째이다. 15세 사춘기 아이들의 사망의 3번째 원인이다.
- 우울증이 있는 아이들의 ⅔는 여러 가지 이유로 정신과 전문의 치료를 받지 않고 있는 실정이다.
- 음주, 알코올 중독, 습관성 약물 남용 등은 우울증으로 인해 생길 수 있지만 그와 반대로 알코올 중독이나 약물 남용으로 인해 우울증이 생길 수 있다.
- 사춘기 아이들의 우울증을 적절히 치료하지 않으면 알게 모르게 우울증 증상이 점점 더 심각해지고 일상생활의 모든 영역에 깊숙이 스며들면서 결국에는 일상생활을 정상적으로 수행하지 못하고 생애가 망쳐질 수 있다.
사춘기 아이들의 우울증 원인
- 우울증 원인은 확실히 모른다.
- 우울증은 위중한 정신병 중 하나이다.
- 우울증은 유전, 생리, 사회, 정신적 요인과 일생 삶에서 받는 스트레스 등이 복합적으로 작용해서 생긴다.
- 우울증이 연령에 관계없이 성인들에게도 소아청소년들에게도 생기고 남녀노소 누구에게도 생길 수 있다.
- 특히 오늘날, 사춘기 아이들은 우울증에 비교적 더 잘 걸린다.
- 우울증이 생기는 원인은 확실히는 모르지만 뇌 속 놀에피네프린(노르에피네프린/Norepinephrine)과 세로토닌(Serotonin)이란 두뇌생화학 물질 대사에 이상이 생길 때 우울증이 생긴다고 믿는다.
사춘기 아이들의 우울증의 유발인자
- 사춘기 여아들은 여러 가지 이유로 우울증에 더 잘 걸리고 그 증상 징후가 여러 가지 형태로 나타날 수 있다.
- 부모의 사망이나 별거, 이혼,
- 가족 일원의 사망,
- 집에서 멀리 떨어져 고독하게 살 때,
- 애인과 헤어질 때,
- 그 외 다른 이유로 우울증이 유발될 수 있다.
- 다시 말하면, 우울증은 복합적 요인에 의해서 유발된다.
- 몇 10년 전까지, 소아들에게는 우울증이 생기지 않는다고 믿었다.
- 그러나 우울증이 오늘날 사춘기 아이들이나 젊은 청년들에게 비교적 흔히 생긴다는 것이 잘 알려졌다.
- 우울증은 사춘기 이전 신생아들, 영유아들, 학령기 아이들에게도 유발될 수 있다.
사춘기 아이들의 우울증의 종류
- 급성형 우울증과
- 만성형 우울증으로도 분류 하고,
- 경도 우울증,
- 중등도 우울증
- 중증 우울증으로도 분류하기도 한다.
- 우울증이 다 나았다가도 재 유발될 수 있다. 이런 우울증은 재발성 우울증이라고 한다.
- 사춘기 아이들의 우울증,
- 성인들의 우울증 등으로 분류할 수 있다.
- 사춘기 아이들에게 스마일링 우울증이 생길 수 있다.
사춘기 아이들의 우울증 발생률
- 15~54세의 미국인 8,000명을 대상으로 우울증 발생률에 관한 미국 NCS 통계에 의하면,
- 중증 우울증을 경험했던 젊은 사람들의 14%는 사춘기 이전부터 우울증이 시작됐었고,
- 경도 우울증을 경험했던 젊은 사람들의 11%는 사춘기가 끝나기 이전부터 우울증이 시작됐다고 한다.
- 9,800명의 미국 6, 8, 9, 10학년 남녀 학생들의 18%에게 우울증이 있었고,
- 여학생들의 25%, 남학생들의 10%에게 우울증이 있었다고 한다. 출처: 미 NICHHDD가 Depression or Bipolar Disorder, Dwight L. Evans, MD and etc.
사춘기 아이들의 우울증의 증상 징후
- 우울증의 주 증상은 느낌장애와 행동장애이고 그로 인해 전반적 건강상태가 이상해진다.
- 나이, 성별, 우울증의 중증도, 우울증의 유발 요인 등에 따라 우울증의 증상 징후가 다양하다.
- 영유아들에게 우울증이 생기면 과도활동장애가 생길 수 있고, 또 대소변을 가리던 영유아가 대소변을 가리지 못하고 퇴행성 행동이 나타나기도 한다.
- 사춘기 아이들이 우울증에 걸리면 부모, 형제, 집안 식구들이나 권위자들에게 반항적 행동을 할 수 있다.
- 특히 사춘기 여아들이 우울증에 걸리면 자기들 신체상 개념이 좋지 않고,
- 자기 자신 모든 것에 관해 실망하고,
- 자기 삶은 실패의 지경에 이르렀다고 생각하고,
- 우울증에 걸리기 전에는 공부하기를 좋아했던 사춘기 아이가 공부를 더 이상 열심히 하지 않고
- 즐겁게 보냈던 사회생활, 육체적 활동과 사회활동에 흥미를 잃고
- 친하던 친구들과 더 이상 어울리지도 않고 혼자서 쓸쓸하게 시간을 보낸다.
- 집중력 결여증(주의력 결핍장애)으로 정신 집중을 잘 할 수 없고,
- 대인관계에도 문제가 생길 수 있다.
- 음식물을 보통 이상으로 더 많이 섭취하거나 보통이상으로 음식물 섭취를 제한 하고
- 자기 체중에 관심을 더 많이 갖는다.
- 부모들이 우울증에 걸리면 자녀들이 우울증에 더 잘 걸릴 수 있다.
- 습관성 약물 남용, 음주, 알코올 중독이나 약물남용으로 인해 우울증이 유발될 수 있다.
- 무분별적이고 난잡하고 복잡한 성관계를 갖고,
- 스트레스를 더 쉽게 받을 수 있고
- 폭력적 행동을 자행할 수 있고
- 가출,
- 무분별한 성관계,
- 십대 임신 등의 문제가 생길 수 있다.
- 부모 자녀 간 대화 문제가 생길 수 있고,
- 학교공부 문제가 생길 수 있다.
- 월경의 주기에 따라 우울 증상이 더 악화되기도 하고 덜 할 수 있다.
- 남여 성별에 관계없이, 무력감, 절망감, 자포자기, 자기비하, 집중력 저하 및 집중력 결핍증, 공상, 권태감, 피곤, 성적부진, 신체적 우울증, 퇴행성 행동, 우울증 발산, 약물 남용, 십대 임신, 범법행위, 자살 등 여러 가지의 우울증의 증상 징후가 생길 수 있다.
- 공부를 잘했던 사춘기 아이들이 우울증에 걸리면 이유 없이 지각, 조퇴, 결석을 자주하고 성적이 점점 떨어지기 시작한다.
- 모든 일에 대하여 과도하게 불평하고,
- 평소 기분이 좋지 않고, 매사에 공격적일 수 있다.
- 잠에 잘 들지 못하거나 자다가 자주 깰 수 있다.
- 꿈을 많이 꾸거나 잠을 너무 많이 잘 수 있다.
- 혼자서 쓸쓸하게 많은 시간을 보내고 친구 사귀기를 싫어한다.
- 우울증에 걸리기 전 매일 열심히 했던 일에 흥미를 점점 잃고
- 무슨 일이든지 아예 시작하지 않으려고 한다.
- 밥맛을 잃고 잘 먹지 않거나 그와 반대로 너무 많이 먹어 비만해질 수 있다.
- 머리가 자주 아프다고 호소하거나
- 배가 자주 아프다고 호소하면서
- 변비가 생길 수 있다.
- 부모나 교사가 무엇이든 물으면 화를 내거나 신경질적으로 대답할 수 있다.
- 이해하기 곤란한 안전사고를 자주 일으키고 사소한 일에 화를 내면서 물건을 때려 부수기도 한다.
- 가택 침입, 물건 파괴 행위 등을 할 수 있다.
- 가끔 죽고 싶다고 말하기도 하며,
- 때로는 실제로 자살 한다.
- 사춘기 아이들의 우울증은 자살의 주원인이 될 수 있다.
- 우울증이 있는 사춘기 아이들은 과음하기도 하고
- 마약이나 습관성 약물에 중독되기도 한다.
- 사춘기 자녀가 우울증으로 그런 유형의 행동을 하는 것을 잘 모르고 있는 부모들이나 대부분의 교사들은 못 된 아이라서 나쁘게 행동하는 줄로 취급할 때도 있다.
- 때문에 부모와 우울증이 있는 자녀와 교사들과 우울증이 있는 학생 사이에 여러 가지 문제가 생길 수 있다.
- 우울증에 걸린 대부분의 사춘기 아이들은 우울증 치료를 곧 받지만 일부는 우울증에 걸린 줄도 모르고, 물론 치료 받지 않고 또 우울증이 있다고 진단을 받고
- 우울증 치료를 받으라고 권장해도 우울증 치료를 받지 않는 사춘기 아이들도 허다하다.
- 우울증은 자살의 주원인이 되고 15~24세 된 사춘기 아이들과 젊은 사람들의 사망의 3번째의 원인이 된다. 그리고 15세 사춘기 아이들의 사망 원인의 3번째의 자살의 원인이라고 이미 언급했다.
- 소아청소년이 심한 우울증을 앓으면 그 후 5년 이내 우울증이 재발될 가능성이 많다.
- 우울증을 적절히 치료하지 않으면 알게 모르게 증상 징후가 점점 심해지고 일상 삶 속에 깊이 스며들면서 결국에는 정상적인 생활을 하지 못하게 된다.
그림 450. 심히 우울한 사춘기 여아.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
사춘기 아이들의 우울증의 진단
- 병력, 증상 징후와 진찰소견 등을 종합해서 우울증을 진단한다.
- 학교 성적이 점차로 떨어지고,
- 학교 수업을 받는 동안 시간이나 집에서도 공상을 하고,
- 모든 것에 흥미를 잃고,
- 혼자 쓸쓸하게 있기를 좋아하며,
- 두통, 복통, 식욕부진, 수면장애, 물건 파괴, 자살 기도 및 자살, 음주, 범법행동 등의 행동장애, 감정 장애, 생각 장애가 있으면 우울증을 진단하는데 큰 도움이 된다.
- 피, 소변, 뇌파, 갑상선 기능의 검사 등으로 우울증과 다른 병들을 감별 진단한다.
- 다음 ①~⑪사항의 우울증의 증상 징후 중 적어도 5가지나 그 이상의 증상들이 동시에 있거나
- 그런 증상 징후가 적어도 2주 이상 계속되거나
- 그런 증상 징후의 중증도가 심하거나
- 그런 증상 징후로 인해 일상생활을 제대로 수행할 수 없으면 우울증이 있다고 진단할 수 있다.
① 죽음에 대한 생각을 하거나, 죽고 싶은 생각을 하거나, 자기는 죽어가고 있다고 생각하기도 하고, 또는 자살을 해서 죽는 방법을 생각하거나, 때로는 자살기도를 한다.
이렇게 죽는 것을 생각하는 우울증의 증상이 나타나면 의사와 즉시 상담하던지 응급실로 데리고 가서 정신과 치료를 받아야 한다.
② 슬프다고 하거나 희망이 하나도 없다고 생각하거나 이유 없이 우는 증상이 계속될 수 있다.
③ 건전한 자존심이 결여되고 아무런 이유도 없이 죄책감에 사로잡히고 나는 더 이상 좋은 사람이 아니라고 느낀다.
④ 살아간다는 것은 아무런 의미도 없고 나에게는 앞으로 더 이상 좋은 것이 생기지 않을 것이라고 생각한다.
⑤ 좋고 나쁘고 즐거운 느낌이 없다.
⑥ 전에 좋아서 많이 했던 공부나 사회활동, 육체활동, 과외활동 등에 흥미를 잃고 절친하게 지냈던 친구들과 더 이상 어울리지도 않고 혼자서 외롭게 시간을 보낸다.
⑦ 무엇을 할 때 결정내리기 어렵고 아예 새로운 일은 시작하지도 않거나 할 수도 없고 기억력이 현재 상실되고 집중력 결여증(주의력 결핍장애)이 생겨 정신집중을 잘 할 수 없다.
⑧ 신경이 예민해지고 사소한 일에 화내고 과잉으로 반응한다.
⑨ 보통 이상으로 잠을 과도히 많이 자거나 적게 잘 수도 있고 보통 이상으로 음식물을 많이 먹거나 적게 먹을 수 있다. 그리고 체중이 비정상적으로 증가되거나 감소된다.
⑩ 특별한 이유가 없이 피로를 항상 느낀다.
⑪ 우울증에 걸린 사춘기 아이들의 일부는 약물남용, 알코올 중독, 무분별적 성관계, 학교 문제, 성적 불량, 가족이나 친구와의 관계에도 문제가 생길 수 있고 권위자들이나 부모들에게 반항적이고 파괴적 행동을 할 수 있다.
사춘기 아이들의 우울증의 치료
- 우울증의 원인, 중증도, 증상 징후에 따라 치료가 다르다.
- 여러 가지 이유와 유발인자로 사춘기 아이들에게 우울증이 유발되어도 우울증을 조기에 정확하게 진단받지 못할 수 있다.
- 적절한 전문가의 도움을 제 때에 받지 못할 수 있다.
- 그래서 우울증에 걸린 사춘기 아이들의 1/4~1/3만 적절한 치료를 받는다고 한다 40.
- 우울증에 걸린 사춘기 아이들을 정신적으로 안정시키고 원인과 유발 인자를 제거해 주는데 전력을 다해야 한다.
- 부모는 의사와 함께 우울증이 있는 사춘기 자녀와 상담하여 우울증을 유발시킨 인자가 무엇인지 알아내야 한다.
- 부모의 자녀 양육 방법이 잘못되어 사춘기 자녀에게 우울증이 생겼을 때는 그 자녀에게 서슴지 말고 사과하고, 잘못된 양육 방법을 곧바로 시정하고, 사춘기 자녀의 생각이 옳으면 생각을 인정해 주어야 한다.
- 우울증이 있는 사춘기 아이가 자살기도를 하거나, 자살을 하겠다고 말할 때는 의사의 지시에 따라 우울증을 응급으로 치료해 주어야 한다.
- 왜냐하면 과거에 한 번이라도 자살기도를 했거나 자살을 하겠다고 말했던 사춘기 아이들의 대부분은 언젠가는 실제로 자살기도를 하든지 자살을 하기 때문이다(자살 참조).
- 이런 이유로 심한 우울증에 걸린 사춘기 아이가 자살을 한다고 말하든지 자살 기도를 하면 병원에 얼마 동안 입원시켜 자살을 예방하기 위해 특별한 관심을 갖고 사춘기 우울증을 치료해 주어야 한다.
- 그밖에 우울증 치료 약물, 심리요법, 상담치료 등으로 우울증을 치료해 준다.
- 여러 가지의 우울증 치료방법 중 가장 중요한 것은 우울증에 걸린 사춘기 아이를 조건 없이 진정으로 사랑해주고 집중적 관심적 사랑을 해 주어야 한다.
- 우울증을 가진 아이와 부모 형제 가족이 다 함께 정신과 전문의의 상담 치료를 받아야 한다.
사춘기 자녀가 우울증에 걸렸다고 의심하거나 진단이 나면
1. 가족들이나 친구들 중 믿을만한 사람에게 우울증에 걸린 것 같다는 사실을 말하고 우울증 치료 전문가나 소아 정신과 전문의와 상담한다.
2. 그렇지 않으면 자기의 단골 소아청소년과 의사의 진단 치료를 곧 받는다.
3. 학교 카운슬러, 간호사, 사회 복지사의 도움을 받는다.
4. 정신과 전문의 도움을 받는다. 가능하면 소아 정신과 전문의의 도움을 받는다.
5. 카운슬링을 해 줄 수 있는 자격을 갖추고 경험 있는 신부, 목사, 또는 랍비의 도움을 받는다.
6. 증상이 더 심해지기 전 우울증 초기에 소아 정신과 전문의의 도움과 치료를 받는 것이 중요하다.
7. 심신이 허약하고 건전한 자존심이 결여되고 학교 공부나 과외활동을 하는데 문제가 생기고 무엇을 잘 해보려고 최선을 다 해 노력하지 않거나 아예 하지 않는 것이 우울증의 증상일 수 있다.
8. 우울증이 있는 사춘기 아이들의 대부분은 카운슬링과 상담 치료나 항 우울증 약으로 잘 치료된다.
9. 우울증은 비교적 흔한 정신병이고 남녀노소 누구에게도 생길 수 있다. 우울증에 걸린 것 같으면 곧 소아 정신과 전문의의 도움과 치료를 받아야 한다.
사춘기 아이들의 우울증 치료 약물
- 우울증 치료에 사용되는 약물에는 Fluoxetine, Paroxetine, Sertraline, Fluvoxamine, Citalopram, Escitalopram, Amitriptyline, Imipramine 등이 있다.
- 그 중 한 종류나 한 종류 이상 항우울증 약물을 선택해서 우울증 치료에 쓸 수 있다.
- 그러나 2008년 2월에 발표한 Irv Kirsch of university of Hull의 연구에 의하면 대부분의 우울증 치료에 쓰는 약물들은 심한 우울증 치료에는 효과가 있으나 경도 우울증 치료에는 별로 효과 없다고 한다. 26, 27, 그 외
- 중증 우울증(Major Depressive Disorder)은 Lexapro(Escitalopram oxalate)로 치료하기도 한다.
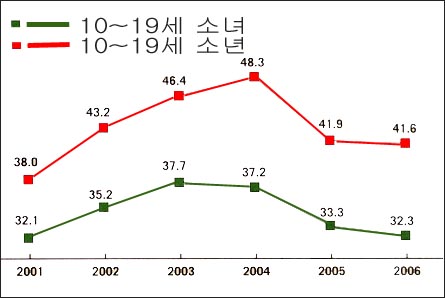
그림2-25. 우울증 치료에 쓰는 항우울증 약물로 치료받는 율은 사춘기 남아들보다 사춘기 여아들에게 더 높다(위 수는 10~19세 사춘기 아이들 1,000명 중 항우울증 약물로 치료받는 아이들의 수).
출처-Medico health solutions inc .and Elsevier Medical news, 2007
항우울제와 불안 제거제(불안 관해제) (I) Antidepressant and Anxiolytics (I)
| 항우 울 제 와 불안 제거제(불안 관해제) 일반 명 | 치료 용량 항우울 제와불 안 제거제 (불안 관해제) 상품명 | 최초 용량(12세 이하) | 유지 용량(12세나 그 이상) | 최초 용량(12세나 그 이상) | 유지 용량(12세나 그 이상) | 부작용 및 참고사항 |
| Fluoxetine | Prozac | 5~10mg/1일 | 10~30mg/1mg | 10mg/1일 | 20~40mg/1일 | 소아 우울증 치료에 가장 많이 쓰고 효과가 있는 항우울중제이다. 치료 시작 14일 전에 MAOI 치료를 시작했으면 이 약을 쓸 수 없다. 위장장애 중추신경계에 부작용, 두통 신경질 진정 등 부작용 |
| Fluoxamine | Luvox | 25mg/1일 | 100~200mg/1일 | 25~59mg/1일 | 150~300mg/1일 | – |
| Paroxetine | Paxil | 5~10mg/1일 | 10~20mg/1일 | 10~20mg/1일 | 20~40mg/1일 | 자반증, 저나트리움증 등 약물 부작용. 여러 다른 종류의 약과 상호 작용을 할 수 있음 |
| Sertraline | Zoloft | 25mg/1일 | 100~150mg/1일 | 25~50mg/1일 | 150~200mg/1일 | 자반증, 저나트리움증 등 약물 부작용. 여러 다른 종류의 약과 상호 작용을 할 수 있음 |
| Citalopram | Celexal | – | 10~20mg/1일 | – | 10~40mg/1일 | Fluoxetine 참조 |
| Venlafaxine | Effexor | 37.5mg/1일 | 75~150mg/1일 | 37.5~75mg/1일 | 150~300mg/1일 | 구기, 현기, 졸음, 변비 등 부작용 |
| Nefazodone | Serzone | – | 50mg 1일 2회 치료를 시작한다. 진찰효과를 관찰하면서 매 3일마다 50mg을 증가한다. 12세 이하 소아의 최대 용량은 1일 300mg이다. | – | 12세 이상 소아의 최대 용량은 1일 600mg/1일 | 5-HT 차단제, 구기 현기 음경 발기 구강적조, 시력장애 등 |
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.1045-1046
표 2-2. 항우울제와 불안 제거제(불안 관해제) (II) Antidepressants and Anxiolytics (II)
| 항우울제 와 불안 제거약(불안 관해제) 일반 명 | 치료 용량 항우울 제와 불안 제거약(불안 관해제) 상품명 | – | – | 용량(18세나 그 이상) | – | 부작용 및 참고사항 |
| Bupropion 지속 방출제 | Wellbutrin SR | – | – | 100mg을 1일 2회, 3일간 치료하고 부작용이 없고 치료효과가 나면 100mg을 1일 3회(소량으로 매 6시간마다)최대 1일 용량은 450mg, 최대 1회 용량은 150mg | – | 중추신경 자극, 체중변화, 구강건조, 두통,위장장애, 불면증, 경련하는 경우나 시력장애가 있으면 이 약으로 치료할 수 없다. |
| Mirtazapine | Remeron | – | – | 매일 취침 전 15mg으로 치료를 시작하고, 매 1~2주마다 점차로 증가 치료한다. | – | 치료시작하기 전에 시비시(CBC), 간 기능검사를 하고 그 후 주기적으로 추적 검사한다. 입맛이 증가하고 체중 증가, 현기증,구기, 구강 건조, 변비, 수면과다, 혈압이 증가되거나 낮아지는 등의 부작용 |
| Buspirone | BusPal | – | – | 사춘기 전 소아; 2.5~5mg/1일, 그 후 매 3~4일 간격으로 2.5mg/1일 증가해서 치료한다. 1일 최대 용량은 20mg. 사춘기 아이; 5~10mg/1일, 4~4일마다 5mg/1일을 증량해서 치료한다. 최대 1회분 용량은 60mg/1일 | – | 빈맥, 두통, 불면, 혼동, 현기, 위장 장애 등 |
| Trazodone | – | – | – | 소아청소년(1~18세); 1.5~2mg/Kg를 총량으로 계산해서 그1일 총량을 2~3등분해서 경구로 섭취한다. 필요에 따라 매3~4일마다 6mg/Kg를 1일 총량으로 계산해서 1일분을 3등분해서 1회분을 3회 복용한다. 성인은 150mg을 3등분해서1등분을 1일 3회 복용한다. 필요에 따라 더 증량해서 치료할 수 있다. | – | 현기, 졸음, 구강건조, 설사, 빈혈, 허약, 경련 등의 부작용 |
| Imipramine | Topranil | – | – | 사춘기 전 소아; 1.5mg/Kg을 1일 총량으로 계산해서 그 1일 분 총량을 3분해서 1일 3회 경구로 섭취한다. 치료 효과에 따라 매 3~4알마다 1~1.5mg/Kg을 증량해서 치료할 수 있다. 1일 최대 용량은 5mg/Kg이다. 사춘기 아이:25_50mg/Kg를 1일 분 총량으로 계산해서 그 1일 분을 한 번에 경구로 복용하든지 3등분해서 1등분을 1일 3회 경구로 섭취한다. 1일 최대 용량은 200mg이다. | – | 녹내장이 있으면 이 약은 금기이다. MAOI제와 함께 치료에 쓸 수 없다, 현기, 졸음 구강 건조 등의 부작용이 생길 수 있다. |
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.1045-1046
Depression in adolescents(Adolescent depression /Teen depression) 사춘기 아이들의 우울증
Overview of Depression in Adolescent Children
• Depression is one of the most serious mental illnesses, and it can occur to anyone in all walks of life, suffering from young, old, young and old.
• If one suffers from severe depression in childhood and adolescence, there is a high likelihood that the depression will recur within 5 years thereafter.
• Bipolar disorder in pre-adolescent infants, school-age children, and adolescent children has increased 40-fold since 1994 (source; Dr. Mark Olson, The Journal of archives of general psychiatry 2007).
• 1 in 10 children and adolescents can develop depression.
• 4 to 18% of adolescent children develop depression.
• Only 30% of preadolescent children with severe mental illness are receiving adequate treatment.
• It is reported that 50% of adults with severe psychosis began to develop psychosis around the age of 14 (Source: Journal watch pediatrics and adolescent medicine, August 2008. p.769).
• The main symptom, signs of depression
o Feeling disorder and
o It is a behavioral disorder.
o Your mental health condition can worsen overall.
• Most children with depression get appropriate treatment soon, but some do not even know they are depressed. Even their parents don’t even know if their children have depression. As a result, it is common for children with depression to not receive adequate treatment for depression.
• It is common for people not to receive adequate treatment even though they are encouraged to receive adequate treatment.
• Depression in adolescents is a major cause of suicide.
• Suicide is the third leading cause of death in late adolescent children and young people aged 15 to 24. It is the third cause of death among 15-year-old adolescent children.
• ⅔ of children with depression are not receiving treatment by a psychiatrist for various reasons.
• Alcoholism, alcoholism, and addictive substance abuse can be caused by depression, but on the contrary, alcoholism or substance abuse can lead to depression.
• If the depression of adolescent children is not properly treated, symptoms of depression become more and more serious without knowing, and they penetrate deeply into all areas of daily life.
Causes of depression in adolescent children
• The cause of depression is unclear.
• Depression is one of the most serious mental illnesses.
• Depression is caused by a combination of heredity, physiology, social, and mental factors and life-long stress.
• Depression occurs in adults, children and adolescents, regardless of age, and can occur in both men and women of all ages.
• Especially today, adolescent children are relatively more prone to depression.
• Although the cause of depression is not clear, we believe that depression occurs when there is an abnormality in the metabolism of brain biochemicals such as norepinephrine and serotonin in the brain.
Factors of depression in adolescent children
• Adolescent girls are more susceptible to depression for a number of reasons, and the symptoms can take many forms.
• death or separation of parents, divorce,
• the death of a family member,
• When living in solitude far away from home,
• When breaking up with a lover,
• Depression can be triggered for other reasons.
• In other words, depression is triggered by multiple factors.
• Until a few decades ago, it was believed that children do not develop depression.
• However, it is well known that depression is relatively common in adolescent children and young people today.
• Depression can also be triggered in newborns, infants, and school-age children before puberty.
Types of depression in adolescent children
1. Acute type of depression
2. Classified as chronic depression,
3. mild depression,
4. Moderate depression
5. It is also classified as severe depression.
6. Depression can be re-induced even after it is over. This type of depression is called recurrent depression.
7. Depression in adolescent children,
8. It can be classified as adult depression.
9. Adolescent children can develop smiling depression.
The incidence of depression in adolescent children
• According to US NCS statistics on the incidence of depression in 8,000 Americans aged 15-54, • 14% of young people who have experienced severe depression started to have depression before puberty,
• 11% of young people who have experienced mild depression report that depression started before puberty ends.
• 18% of 9,800 male and female students in grades 6, 8, 9 and 10 in the United States had depression,
• It is reported that 25% of female students and 10% of male students had depression. Source: US NICHHDD, Depression or Bipolar Disorder, Dwight L. Evans, MD and etc.
Symptoms, signs of depression in adolescent children
• The main symptoms of depression are feeling disorders and behavioral disorders, which makes the overall health status weird.
• Symptoms of depression vary according to age, sex, severity of depression, and factors that cause depression.
• When depression occurs in infants and toddlers, hyperactivity disorder may occur, and infants and toddlers who have covered their stool may not be able to cover stool and may exhibit degenerative behavior.
• When adolescents become depressed, they can act rebelliously against their parents, siblings, family members, or authorities.
• Especially when adolescent girls suffer from depression, their body concept is not good, • Being disappointed about everything yourself,
• You think your life has reached the point of failure,
• Adolescent children who liked to study before becoming depressed do not study hard anymore.
• Losing interest in social life, physical and social activities that you had enjoyed
• She no longer hangs out with her close friends and spends lonely time alone.
• Can’t concentrate well due to lack of concentration (attention deficit disorder), • Interpersonal problems can also arise.
• Eating more than usual or limiting food intake above normal
• Be more interested in your weight.
• When parents get depressed, their children are more likely to get depressed.
• Depression can be triggered by habitual substance abuse, alcohol use, alcoholism or substance abuse. • having reckless, promiscuous and complex sex,
• You can get stressed more easily
• be able to commit violent behavior
• run away,
• reckless sex,
• Problems such as teenage pregnancy may occur
. • There may be communication problems between parents and children,
School study problems may arise.
• Depending on the menstrual cycle, depressive symptoms may get worse or worse.
• Regardless of gender, helplessness, despair, desperation, self-deprecation, decreased concentration and concentration deficit, daydreaming, boredom, tiredness, sluggishness, physical depression, degenerative behavior, emanating depression, substance abuse, teenage pregnancy, criminal behavior, suicide There are many signs of depression, including symptoms of depression.
• When adolescent children who have studied well become depressed, they often tarry, leave early, and absent from school for no reason, and their grades begin to decline.
• complaining excessively about everything,
• You usually don’t feel well and can be aggressive in everything. • Difficulty falling asleep or waking up frequently during sleep.
• You can dream a lot or sleep too much.
• I spend a lot of time alone and hate making friends.
• I gradually lose interest in what I did hard every day before I became depressed.
• Try not to start anything at all.
• Losing the taste of rice and not eating well, or vice versa, can lead to obesity due to eating too much.
• Complaining that your head hurts often • Complaining that your stomach hurts often
• Constipation may occur.
• If a parent or teacher asks anything, it can be angry or nervous.
• Often causes hard-to-understand safety accidents, gets angry at trivial things, and strikes them apart.
• They can intrude into houses or destroy objects.
• Sometimes they say they want to die,
• Sometimes they actually commit suicide.
• Depression in adolescent children can be a major cause of suicide. • Adolescent children with depression may drink too much
• You are also addicted to drugs or addictive drugs.
• Parents and most teachers who are unaware of their adolescent’s depressive behaviors are sometimes treated as bad behaviors because they are bad children.
• Because of this, a number of problems can arise between parents and depressed children and teachers and depressed students.
• Most adolescent children with depression get treatment for depression soon, but some do not even know that they have depression, and of course, they are diagnosed with depression without treatment.
• Many adolescent children do not receive treatment for depression even though they are encouraged to seek treatment for depression.
• Depression is the leading cause of suicide and is the third leading cause of death in adolescents and young people aged 15 to 24 years old. And it has already been mentioned as the third leading cause of suicide among 15-year-old adolescent children.
• If a child or adolescent suffers from severe depression, there is a high likelihood that the depression will recur within 5 years.
• If depression is not treated appropriately, symptoms of symptoms become more and more severe without you knowing, and they penetrate deeply into your daily life, eventually preventing you from living your normal life.
Figure 450. A teenage girl who is very depressed. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Diagnosis of depression in adolescent children
• Diagnosis of depression by synthesizing medical history, symptom signs and examination findings.
• school grades gradually decline,
• Daydreaming at home or at home while in school,
• losing interest in everything,
• likes to be lonely alone,
• Headache, abdominal pain, loss of appetite, sleep disturbances, object destruction, suicidal attempts and suicides, behavioral disorders such as alcohol and criminal behavior, emotional disorders, and thought disorders are very helpful in diagnosing depression.
• Differentially diagnose depression and other diseases by testing blood, urine, brain waves, and thyroid function.
• At least 5 or more of the symptoms of depression in the following items ①~⑪ are present at the same time or
• signs of such symptoms persist for at least two weeks or
• The severity of the signs of such symptoms is severe or
• Depression can be diagnosed if you are unable to perform your daily activities properly due to signs of such symptoms.
① I think about death, I think I want to die, I think I am dying, I think about how to die by committing suicide, and sometimes I pray suicide. If you experience symptoms of depression thinking about dying like this, you should consult your doctor immediately or take you to the emergency room for psychiatric treatment.
② Symptoms of sadness, thinking that there is no hope, or crying for no reason may continue.
③ Lack of sound pride and guilty for no reason, I feel that I am no longer a good person.
④ Living is meaningless and I think there will be no more good things in the future
⑤ There is no good, bad, or pleasant feeling.
⑥ I lost interest in studying, social activities, physical activities, extracurricular activities, etc. I liked a lot before, and I no longer hang out with my close friends and spend time alone alone.
⑦ It is difficult to make a decision when to do something, you can’t start or do anything new, your memory is currently lost, and you have a lack of concentration (attention deficit disorder), so you can’t concentrate well.
⑧ Nervousness becomes sensitive, gets angry at trivial things, and reacts excessively.
⑨ You may sleep too much or sleep less than usual, and you may eat more or less food than usual. And weight is abnormally increased or decreased.
⑩ I always feel tired for no specific reason. ⑪ Some of the depressed adolescent children may have substance abuse, alcoholism, indiscriminate sex, school problems, poor grades, problems with family and friends, and may be rebellious and destructive to authorities or parents.
Treatment of depression in adolescent children
• Treatment varies depending on the cause, severity, and symptoms of depression.
• Depression may not be diagnosed early and accurately even if depression is induced in adolescent children for various reasons and triggers.
• You may not be able to get the right expert help on time.
• So, only 1/4 to 1/3 of depressed adolescent children are said to receive adequate treatment 40. • We must do our best to mentally stabilize depressed adolescent children and eliminate causes and triggers.
• Parents should consult with their doctors with their depressed adolescent children to find out what triggers the depression.
• When a parent’s child-rearing method is wrong and adolescent children become depressed, do not hesitate to apologize to the child, correct the wrong parenting method immediately, and accept the adolescent child’s thoughts if they are correct.
• When a depressed adolescent child prays to commit suicide or commits suicide, the depression should be treated as an emergency according to the doctor’s instructions.
• Because most of the adolescent children who have committed suicide at least once in the past or who have said they will commit suicide will one day actually commit suicide or commit suicide (see Suicide).
• For this reason, if adolescents with severe depression say they commit suicide or attempt suicide, they should be hospitalized for a while and treated with special attention to prevent suicide.
• In addition, depression treatment drugs, psychotherapy, and counseling treatment are used to treat depression.
• Among the various treatment methods for depression, the most important thing is to truly love the depressed adolescent child without condition and give intensive love.
• Children with depression and their parents, siblings, and family members should both seek counseling from a psychiatrist.
If you suspect or diagnose that your adolescent child has depression,
1. Tell your family or friends that you think you are depressed and talk to a depression treatment specialist or pediatric psychiatrist.
2. Otherwise, you will receive diagnosis and treatment from your regular pediatrician soon.
3. Seek help from school counselors, nurses, and social workers.
4. Get help from a psychiatrist. If possible, seek help from a pediatric psychiatrist.
5. Seek the assistance of a priest, pastor, or rabbi who is qualified and experienced in counseling.
6. It is important to seek the help and treatment of a pediatric psychiatrist in the early stages of depression before symptoms worsen.
7. Depression can be symptoms of weakness in mind and body, lack of sound self-esteem, problems with schoolwork or extracurricular activities, and not trying to do best or not at all.
8. Most of depressed adolescent children are well treated with counseling, counseling, or antidepressant medications
. 9. Depression is a relatively common psychosis and can occur in both men and women of all ages. If you think you are depressed, you should immediately seek help and treatment from a pediatric psychiatrist.
Drugs to treat depression in adolescent children
• Drugs used to treat depression include Fluoxetine, Paroxetine, Sertraline, Fluvoxamine, Citalopram, Escitalopram, Amitriptyline, and Imipramine.
• You can choose one or more antidepressant drugs to treat depression.
• However, according to a study by Irv Kirsch of the University of Hull published in February 2008, most of the drugs used to treat depression are effective in treating severe depression, but not very effective in treating mild depression. 26, 27, others
• Major Depressive Disorder is sometimes treated with Lexapro (Escitalopram oxalate).
Figure 2-25. The rate of treatment with antidepressant drugs used to treat depression is higher among adolescent girls than among adolescent boys (the number above is the number of children treated with antidepressant drugs out of 1,000 adolescent children aged 10-19 years). Source-Medico health solutions inc .and Elsevier Medical news, 2007
Antidepressant and Anxiolytics (I) Antidepressant and anxiety remover (anxiety remission agent) 항우울제와 불안 제거제(불안 관해제) (I) Antidepressant and Anxiolytics (I)
| Antidepressant drugs and anxiety-relieving drugs | Treatment capacity Antidepressant and anxiety remover (anxiety remission agent) |
Initial dose (12 years old or younger)
|
The maintenance dose (12 years old or older) | The first dose (12 years old or older) | The maintenance dose (12 years old or older) | side effects and note |
| Fluoxetine | Prozac | 5~10mg/a day | 10~30mg/1mg/a day | 10mg/a day | 20~40mg/a day | It is the most used and effective antidepressant for the treatment of depression in children. If you start MAOI treatment 14 days before the start of treatment, you cannot use this drug. Side effects on the central nervous system with gastrointestinal disorders, headaches, nervous sedation, etc. |
| Fluoxamine | Luvox | 25mg/a day | 100~200mg/a day | 25~59mg/a day | 150~300mg/a day | – |
| Paroxetine | Paxil | 5~10mg/a day | 10~20mg/a day | 10~20mg/a day | 20~40mg/a day | Drug side effects such as purpura and hyponatrium. May interact with many different types of drugs |
| Sertraline | Zoloft | 25mg/a day | 100~150mg/a day | 25~50mg/a day | 150~200mg/a day | Drug side effects such as purpura and hyponatrium. May interact with many different types of drugs |
| Citalopram | Celexal | – | 10~20mg/a day | – | 10~40mg/a day | See Fluoxetine |
| Venlafaxine | Effexor | 37.5mg/a day | 75~150mg/a day | 37.5~75mg/a day | 150~300mg/a day | Side effects such as nausea, dizziness, drowsiness, and constipation |
| Nefazodone | Serzone | – | Start 50mg treatment twice a day. Increasing 50mg every 3 days while observing the examination effect. The maximum dose for children under 12 years of age is 300mg per day. | –The maximum dose for children 12 years of age or older is 600mg/day. | 5-HT blocker, vertigo, penis erection, oral redness, visual impairment, etc. |
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.1045-1046
표 2-2. 항우울제와 불안 제거제(불안 관해제) (II) Antidepressants and Anxiolytics (II)
| 항우울제 와 불안 제거약(불안 관해제) 일반 명 | Treatment dose Antidepressant and anxiety-relieving drug (anxiety remission) | – | – | Dose (18 years old or older) | – | Side effects and notes |
| Bupropion 지속 방출제 | Wellbutrin SR | – | – | If 100mg is treated twice a day for 3 days, and there is no side effect and there is a therapeutic effect, 100mg is treated 3 times a day (every 6 hours in small doses), the maximum daily dose is 450mg, and the maximum one dose is 150mg. | – | Central nerve stimulation, weight change, dry mouth, headache, gastrointestinal disorder, insomnia, convulsions, or visual impairment cannot be treated with this drug. |
| Mirtazapine | Remeron | – | – | Start treatment with 15mg every day before bedtime, and gradually increase treatment every 1-2 weeks. | – | Before starting treatment, during fertilization (CBC), liver function tests are performed, and follow-up tests are performed periodically thereafter. Side effects such as increased appetite, weight gain, dizziness, goji, dry mouth, constipation, excessive sleep, increased or decreased blood pressure, etc. |
| Buspirone | BusPal | – | –Children before puberty; Treatment is 2.5~5mg/1 day, increasing 2.5mg/1 day every 3~4 days thereafter. The maximum daily dose is 20mg. Adolescent child; 5~10mg/1 day, every 4~4 days, increase the amount of 5mg/1 day to treat. The maximum dosage is 60mg/day | – | Tachycardia, headache, insomnia, confusion, dizziness, gastrointestinal disorder, etc. | |
| Trazodone | – | – | –Children and adolescents (1-18 years old); Calculate 1.5~2mg/Kg as the total amount, divide the total amount per day into 2~3 equals, and take it orally. If necessary, calculate 6mg/Kg as the total amount per day every 3-4 days, divide the daily supply into 3 equal portions, and take 1 dose 3 times. Adults divide 150mg into 3 parts and take 1 part 3 times a day. If necessary, it can be further increased and treated. | – | Side effects such as dizziness, drowsiness, dry mouth, diarrhea, anemia, weakness, and convulsions | |
| Imipramine | Tofranil | – | – | Children before puberty; Calculate 1.5mg/Kg as the total amount per day, divide the total amount per day into 3 minutes and take it orally 3 times a day. Depending on the treatment effect, it can be treated by increasing 1 to 1.5 mg/Kg every 3 to 4 tablets. The maximum daily dose is 5mg/Kg. Adolescent children: Calculate 25_50mg/Kg as the total amount per day, and take the daily portion orally at a time, or take it into 3 equal portions and take it orally 3 times a day. The maximum daily dose is 200mg. | – | If you have glaucoma, this drug is contraindicated. It cannot be used for treatment with MAOI drugs, it may cause side effects such as dizziness, drowsiness, and dry mouth. |
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.1045-1046
출처와 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제7권 소아청소년 감염병
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Nelson textbook, 15 edition. PDR 63th ed, 2009
-
Manual of emergency pediatrics 4th edition, Robert M. Reece, M.D., p.155, 160, 426
-
Emergency Pediatrics, A guide to ambulatory care, 5th edi. Roger M. Barkin, Peter Rosen, p.761, 758, 175
-
Quick Reference to Pediatric Emergencies, Delmer J. Pascoe, M.D., Mose Grossman, M.D., p.
-
Nelson textbook, 14th edition p.525-526
-
The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition, p.131, 730, 837, 842, 859-860, 1045-1046, 922-923
- Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
- The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
- Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Manual of Emergency Care
- 응급환자관리 정담미디어
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- Neonatal Resuscitation American heart Association
- Neonatology Jeffrey J.Pomerance, C. Joan Richardson
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
- Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
- Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- Handbook of Pediatric Neurology, Katherine B. Sims, MD
- 소아과학 대한교과서
- 제1권 소아청소년 응급의료 참조문헌과 출처
- Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”