류마티스 열(류머티스 열) Rheumatic fever
류마티스 열(류머티스 열)의 개요
- A군 연쇄상구균 감염으로 생긴 편도염, 인두염, 인두 편도염, 중이염, 또는 성홍열 등을 앓는 중이나, 다 나은 후에 A군 연쇄상구균 항원 항체 이상반응으로 체내 결합조직이나 심장 등 신체 여러 계통의 여러 기관에 생기는 염증을 류마티스 열, 류머티스 열 또는 류머티스성 열이라고 한다.
- A군 베타 용혈성 연쇄상구균을 편의상 여기서 A군 연쇄상구균이라고도 한다.
류마티스 열(류머티스 열)의 원인
- A군 연쇄상구균 급성 편도염이나 인두 편도염, 임두염 또는 다른 여러 가지의 A군 연쇄상구균 감염병이 신체 어떤 부위에 있을 때 A군 연쇄상구균 항원 항체 이상반응으로 결합조직에 염증이 생겨 류마티스 열이 생긴다.
- 류마티스 열이 발병되기 바로 전이나 발병될 당시에 신체의 어느 부위에 A군 연쇄상구균 감염에 의한 감염병이 있는 것이 보통이다.
- 드물게 A군 연쇄상구균에 의한 감염병을 최근에 앓았던 병력도 없고 류마티스 열 발병 당시 A군 연쇄상구균 감염병을 앓고 있지 않을 수 있다.[부모도 반의사가 되어야 한다-소아가정간호백과]-제7권 소아청소년 감염병-A군 연쇄상구균에 의한 감염병, 소아청소년 호흡기 질환-인두염, 편도염, 인두 편도염 참조.
류마티스 열(류머티스 열)의 증상 징후

- 류마티스 열의 주증(동반 질환)에 따라, 류마티스 열의 진행 과정, 합병증의 유무, A군 연쇄상구균 감염에 의한 전염병의 종류 등에 따라 증상 징후가 많이 다르다.
-
류마티스 열에 걸렸을 때
-
류마티스 심장염,
-
류마티스 관절염,
-
류마티스 피부 발진,
-
유주성 홍반(가장자리 홍반),
-
류마티스 무도증,
-
류마티스 결절(피하 결절),
-
류마티스 폐렴 등 주 동반 질환이 생길 수 있다.
-
-
앞서 열거한 이런 류마티스 열로 생긴 류마티스 심장염, 류마티스 관절염, 류마티스 피부 발진(유주성 홍반), 류마티스 무도증, 류마티스 결절을 류마티스 열의 주 동반 질환 또는 류마티스 열의 주증 이라고 한다.
-
류마티스 열을 앓을 때 언제든지 이런 류마티스 열의 주 동반 질환이 한꺼번에 다 나타나는 것이 아니다.
-
그 중 한 가지 주 동반 질환이나 몇 가지 또는 거의 모든 류마티스 열의 주 동반 질환이 다 나타날 수 있다.
-
류마티스 열은 A군 연쇄상구균 감염에 의해 생기는 인두염, 편도염, 인두편도염, 성홍열 등이 더 잘 발생되는 겨울철과 봄철에 더 많이 나타난다.
-
A군 연쇄상구균에는 여러 균종이 있는데 그 중 류마티스 열을 일으키는 균종이 따로 있다.
-
3세 이전 영유아들이나 3세 이후 유아들, 학령기 아이들이나 사춘기 아이들, 성인들도 류마티스 열에 걸릴 수 있지만 5∼15세 연령층 소아청소년이 더 잘 걸릴 수 있다.
-
또 위생시설이 불결한 환경에서 사는 아이들이나 협소 거주지에서 사는 소아청소년들이 이 병에 더 잘 걸릴 수 있다.
-
A군 연쇄상구균 감염병을 앓는 환아들의 3%에서 류마티스 열이 발생할 수 있다고 하나 일정한 시기와 장소 등에 따라 집중적으로 더 많이 발생될 수 있다.
-
그래서 류마티스 열의 전반적인 발생 율은 0.3%에 불과하다고 한다.
-
대부분 A군 연쇄상구균 감염에 의한 전염병을 앓은 후 약 1∼5주일 경에 류마티스 열의 주 동반 질환(주증) 중 하나 또는 하나 이상 여러 개 주 동반 질환이 발생되는 것이 보통이다.
-
그렇지만 류마티스 무도증은 A군 연쇄상구균 감염에 의한 전염병을 앓은 후 2∼6개월이 지난 후에도 발생될 수 있다.
-
A군 연쇄상구균 감염에 의한 인두염이나 편도염 등에 의해서 생기는 증상 징후와 류마티스 열에 의해서 생기는 증상 징후가 같이 나타날 수 있다.
-
또 류마티스 열을 앓을 때 어떤 종류의 주 동반 질환에 따라 증상 징후가 다르다.
-
류마티스 관절염, 류마티스 무도증, 류마티스 심장염, 류마티스 결절 등에서 생기는 증상 징후가 동시에 나타날 수 있다.
-
류마티스 열이 있을 때 맹장염의 증상 징후와 비슷한 복통이 생길 수 있고, 또 미열이나 고열 등 증상 징후가 생길 수 있다.
-
이런 증상 징후는 거의가 급성으로 오는 것이 보통이지만 때로는 서서히 만성으로 나타나기도 한다.
- 류마티스 열의 각 동반 질환에 관해 다음 각항에서 더 자세히 설명한다.
1. 류마티스 심장염 Rheumatic carditis
그림 78. 류마티스 심장염을 앓을 때
의사의 지시에 따라 육체적, 정신적 안정을 취해야한다.
Copyright ⓒ 2011 John Sangwon Lee, M.D.. FAAP
- 류마티스 열을 처음 앓는 소아청소년들 중 40% 정도는 류마티스 열에 걸리면 류마티스 열의 주 동반 질환들의 하나인 류마티스 심장염이 생길 수 있다.
- 어떤 경우는 류마티스 열의 다른 주 동반 질환은 하나도 없는데 류마티스 심장염만 앓을 수 있다.
- A군 베타 용혈성 연쇄상구균을 편의상 A군 연쇄상구균이라 칭한다.
- A군 연쇄상구균 인두염 등을 앓다가 류마티스 관절염이나 류마티스 열의 다른 주증들이 나타나면서 1~2일 동안 앓다가 류마티스 심장염이 나타날 수 있다.
- 류마티스 심장염은 류마티스 열의 주 동반 질환의 하나이다.
- 류마티스 심장염이 있으면 심장내막과 심장 근육이 손상된다. 그래서 류마티스 심내막염도 생길 수 있다.
- 좌심방과 좌심실 사이에 있는 승모판이나 좌심실과 대동맥 사이에 있는 대동맥판의 폐쇄, 또는 승모판이나 대동맥 판 부전증이 생길 수 있다.
- 심장을 둘러싸고 있는 심낭 강 속에 체액이 고일 수 있다. 이 병이 경미하게 생길 때는 아무 증상 징후가 거의 나타나지 않을 수 있다. 이런 병이 있는지 모르고 지내기도 한다.
- 류마티스 심장염이 경미하게 생겼을 때는 체중이 감소되고 입맛이 떨어지면서 짜증을 잘 내는 정도 증상 징후만 나타날 수 있다.
- 류마티스 심장염이 심할 때는 심장이 비정상적으로 커지고 심장 내막염과 심부전증이 생길 수 있다.
- 심장 박동이 빠르고 비정상 심잡음이 들릴 수 있다.
- 이런 류마티스 심장염을 조기에 적절하게 치료하지 않으면 몇 주 내지 몇 달 동안 계속 앓을 수 있다.
- 류마티스 심장염을 앓고 난 후 수개월 내지 수년이 지난 후 심장의 승모판이나 대동맥판 등이 단단히 굳어지고 좁아지며 쪼그라질 수 있다.
- 승모판과 대동맥판이 비정상적으로 좁아지며 작아질 수 있다.
- 이때 숨이 많이 가쁘고, 왼쪽 앞가슴이 울렁거리며, 심장 박동이 빠르게 뛸 수 있다.
- 류마티스 심장염이 심해지면 폐 속에 공기가 정상적으로 차 있는 대신 피와 체액이 괴는 울혈성 심장부전증이 생기고 기침을 많이 하며 숨이 더욱 더 가쁘게 된다.
- 심장염이 계속 더 진행되면 생명까지 위험하게 된다.
2. 류마티스 관절염 Rheumatic arthritis

사진 79. 심한 A군 베타 용혈성 연쇄상구균성 인두염과 편도염.
붓고 빨간 편도에 곱이 끼어 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 80. 심한 A군 베타 용혈성 연쇄상구균성 인두염과 편도염.
붓고 빨간 편도에 곱이 끼어 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
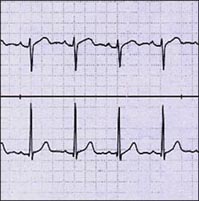
그림 81. 정상 심전도 검사.
심장에 이상이 있나 알아보기 위해 심전도 검사를 한다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
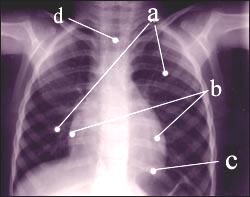
사진 82. 가슴 X-선 사진
심장에 이상이 있나 알아보기 위해 가슴 X-선 사진 검사를 한다. a-폐, b-심장, c-횡격막, d-기관. Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
- 류마티스 열을 앓는 아이들 중 75% 정도 류마티스 열의 주 동반 질환인 류마티스 관절염을 앓는다.
- 류마티스 관절염을 앓을 때 관절이 확연히 붓지 않고 관절 통증만 있을 때도 있다.
- 팔꿈치 관절, 손목관절, 발목관절, 무릎 관절 등과 같이 비교적 큰 관절들 중 한 개의 관절이나 둘, 또는 그 이상 여러 개의 관절에 류마티스 관절염이 동시 생길 수 있다.
- 이 병이 있으면 관절이 갑자기 빨갛게 부을 수 있고 따뜻해진다. 그 관절을 조금만 움직이거나 살살 만지기만 해도 심하게 아픈 것이 류마티스 관절염의 특징이다.
- 손에 있는 손 관절이나 발에 있는 목 관절, 고관절도 류마티스 관절염이 드물게 생길 수 있다.
- 류마티스 관절염이 있을 때 여러 관절이 동시에 아플 수 있지만 붓지 않을 수 있고, 여러 개의 관절이 동시에 붓고 아플 수 있다.
- 류마티스 관절염이 한 개의 관절에 생겨 갑자기 붓고 심하게 아프다가 얼마 후에 다 나은 것 처럼 관절염의 증상 징후가 갑자기 다 없어질 수 있다.
- 거의 비슷한 증상 징후를 가진 관절염이 다른 관절로 옮겨가는 이동성 다발성 류마티스 관절염도 생길 수 있다.
- 류마티스 관절염을 적절히 치료해 주면 관절염이 있던 관절에 후유증도 남기지 않고 잘 낫는 것이 이 병의 특징 중 하나이다.
3. 류마티스 결절(류마티스 피하 결절 Rheumatic nodules
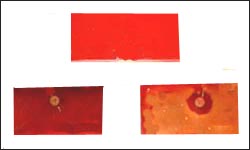
사진 83. 상-A군 베타 용혈성 연쇄상구균을 세균배양하기 위해 인큐베이터에 넣기 전 인두점액을 묻힌 혈액 우무 배양지, 하좌-A군 연쇄상구균이 아닌 인두 상존 잡균이 자란 세균 혈액 우무 배양지, 하 우-A군 베타용혈성 연쇄상구균(A군 연쇄상구균)이 자란 세균 혈액 우무 배양지
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
사진 84. 상-세균배양 인큐베이터에서 인두 상존 잡균이 자란 세균 혈액 배양지, 하-A군 연쇄상구균이 자란 세균 혈액 우무 배양지
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 85. A군 연쇄상구균 항원항체 응집반응검사가 음성으로 나타난 것
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 86. A군 연쇄상구균 항원항체 응집반응검사가 양성으로 나타난 것
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
- 류마티스 열을 앓을 때 관절의 부위에 있는 피하 조직에 생긴 단단한 결합조직 멍울을 류마티스 피하결절 또는 류마티스 결절이라고 한다.
- 류마티스 결절은 류마티스 열의 주 동반 질환 중 하나이다.
- 류마티스 결절의 크기는 쌀알만 한 것도 있고 메주콩알만 것도 있다.
- 만져도 아프지 않은 것이 보통이다.
- 류마티스 관절염이 재발될 때나 류마티스 심장염이 좀 더 심할 때 류마티스 결절이 더 잘 생길 수 있다.
- 류마티스 결절 자체가 건강 문제를 더 일으키지는 않지만 환자가 더 심한 류마티스 열을 앓고 있다는 조짐으로 볼 수 있다.
- 류마티스 열을 앓을 때 류마티스 결절의 유무는 임상적으로 중요한 가치가 있다.
- 류마티스 열을 앓는 아이들 중 5∼10%에 류마티스 결절이 나타난다.
- 이 류마티스 결절은 류마티스 열을 앓기 시작한 몇 주 후에 나타나는 것이 보통이다.
4. 류마티스 유주성 홍반(유연성 홍반/가장자리 홍반)Rheumatic erythema marginatum

사진 87. 유주성 홍반(유연성 홍반, 가장자리 홍반)
이 사진은 라임병의 유주성 홍반이다.
Copyright ⓒ 2011 John sangwon Lee, M.D.. FAAP
- 류마티스 열이 있는 환아 중 5∼10% 정도 류마티스 유주성 홍반이 나타날 수 있다. 류마티스 유주성 홍반은 유주성 홍반 또는 가장자리 홍반이라 한다.
- 류마티스 유주성 홍반은 류마티스 열의 주 동반 질환들 중 하나이다.
- 라임 병 등 다른 병이 있을 때도 류마티스 유주성 홍반과 거의 비슷한 피부 발진이 나타날 수 있다.
- 이 발진이 나타나면 류마티스 열을 진단하는데 도움이 되지만 중증도에는 별 관련이 없다.
- 류마티스 유주성 홍반은 조금 붉고 표면이 조금 부어오르나 가렵지는 않다. 발진의 가장자리는 파도 같이 굴곡이 있고 좀 뚜렷하며 둥그스름하다.
- 이 발진은 몸통과 팔다리 부위에 더 자주 나타날 수 있고 나타났다 없어지고 다시 나타나는 경향이 있다.
5. 류마티스 무도증(舞蹈症)Rheumatic Chorea
- 무도증은 류마티스 열의 주 동반 질환들 중 하나이다.
- 무도증을 류마티스 무도증이라고도 한다.
- 류마티스 무도증이 있으면 한쪽 얼굴, 양쪽 얼굴, 팔 등을 목적이 없이 비율동적이고 순서 없이 춤추는 듯이 움직이기도 한다.
- 무도증은 류마티스 열의 다른 주 증상들과 함께 나타날 수 있고, 따로 나타날 수 있다.
- 무도증의 증상이 나타나면 갑자기 춤추는 듯이 움직여지며 그때 몸을 의식적으로 제지할 수 없어서 자기 몸을 손상시킬 수 있다.
- 글씨를 쓰거나 말을 하는 데도 지장이 생기고 정서적으로 불안해서 갑자기 울다 웃는 정서 이상이 나타날 수 있다.
- 적절히 치료를 해 주지 않으면 몇 주일, 몇 달, 또는 1년 동안 계속 될 수 있다.
6. 류마티스 폐렴 Rheumatic pneumonia
- 류마티스 열이 있을 때 류마티스 폐렴 등 동반 질환이 생길 수 있다.
- 류마티스 폐렴은 박테리아나 바이러스 등 병원체가 폐에 직접 감염되어 폐에 생긴 감염병이 아니고, A군 베타 용혈성 연쇄상구균 항원 항체 이상반응으로 생기는 폐렴이다.
류마티스 열의 진단
- 류마티스 열은 한 번 앓고 낫는 병이 아니라 다 나은 후에 재 유발될 수 있으므로 계속 예방 치료를 잘 해야 한다. 진단을 확실히 하는 것이 중요하다
- 류마티스 열은 재발될 수 있기 때문에 류마티스 열 재발하지 않게 꼭 예방해야 한다. 류마티스 폐렴을 처음부터 정확히 진단하고 또 류마티스 열도 진단하고 치료해야 한다.
- 류마티 열과 류마티 폐렴이 재발되지 않게 예방해야 한다.
- 병력, 증상 징후, 진찰소견 등을 종합해서 류마티스 열이 의심되면 병원에 입원하여 진단 치료를 받는 것이 보통이다.
- 인두 편도 점막층에서 채취한 점액 피검물로 A군 베타 용혈성 연쇄상구균 세균배양검사 및, 또는 A군 베타 용혈성 연쇄상구균 항원 항체 응집 반응검사를 해서 진단한다.
-
- 그 밖에 ASO 피검사,
- ESR 검사,
- 심전도 검사,
- CPR 검사,
- 가슴 X-선 사진검사,
- 심장 초음파 검사 등을 하고 그 외 적절한 다른 여러 종류의 검사로 진단한다.
- 아스피린은 류마티스 열을 치료하는데 특효약이다. 그러나 류마티스 열을 앓고 있는지 확실히 모르는 상태에서 아스피린으로 치료하면 류마티스 열로 생기는 증상 징후는 금방 좋아질 수는 있지만 류마티스 열을 조기에 확진하는 데 지장을 준다.
- 병은 잘 낫는 것 같지만 예방을 소홀히 하면 재발을 될 수 있다.
- 류마티스 열로 인해 관절염이나 심장염이 생겼는지 다른 병으로 생겼는지 의사의 확실한 진단과 처방 없이 함부로 아스피린 등 항염증제나 해열제로 치료해서는 안 된다.
- 류마티스 열의 진행 과정, 각 주 동반 질환의 정도에 따라 치료가 다르다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제11권 소아청소년 심장 혈관계 질환-류마티스 열 참조.
류마티스 열의 일반적 치료 Gentral treatment of rheumatic fever
1. 정신적·육체적 안정을 취한다.
- 류마티스 열의 주 동반 질환의 정도, 진행과정, 나이 등에 따라 진단 치료를 다르다.
- 류마티스 심장염의 중증도에 따라 정신적 육체적 안정을 취하는 것은 중요한 치료이다
- 심하게 앓을 때는 대소변을 실내에서 누게 하고 음식물도 침상에서 먹도록 육체적 안정을 취해야 한다.
- 류마티스 심장염을 앓을 때는 3주~3개월 동안 정신적, 육체적으로 안정을 취하게 하는 것이 상당히 중요하다.
- 류마티스 열의 주 동반 질환들 중 하나인 류마티스 심장염이 생기지 않은 류마티스 열을 앓을 때는 치료 시작한 후 7∼10일쯤에 중증도가 호전되고 기분과 기력이 좋아지면 육체적 기동을 점차로 서서히 하기 시작해도 된다.
2. 의사의 처방에 따라 아스피린으로 치료한다.
- 류마티스 열은 아스피린으로 치료할 수 있고, 필요에 따라 아스피린과 프레드니손제 두 가지 약물로 치료 한다.
- 류마티스 열을 치료할 때 아스피린의 치료용량은 다른 질환을 아스피린으로 치료할 때의 아스피린 치료 용량보다 훨씬 높은 용량으로 치료한다.
- 아스피린으로 치료를 할 때 이명증, 위장장애, 그밖에 다른 여러 가지 부작용, 약물 유해작용이 생길 수 있다.
- 아스피린으로 적어도 10일 정도 치료하다가 중증도가 호전되면 더 이상 아스피린 치료를 하지 않아도 된다.
- 프레드니손제로 치료할 때도 많은 부작용이 생길 수 있고 일반적으로 4∼6주 정도 치료한다.
3. 류마티스 열은 A군 베타 용혈성 연쇄상구균에 의해서 생긴 인두염 및, 또는 편도염 등을 앓는 도중이나 앓은 후에 발생할 수 있다.
- 먼저 A군 베타 용혈성 연쇄상구균 감염에 의한 전염병이 있는지 확인해야 한다.
- 인두나 신체의 다른 부위에 있는 감염병 병소에서 얻은 점액 피검물로 A군 베타 용혈성 연쇄상구균 세균배양검사를 해서 그 결과에 따라 류마티스 열을 진단할 수 있다.
- 류마티스 열을 앓을 때 세균배양검사에서 A군 베타 용혈성 연쇄상구균이 배양되지 않아도 페니실린이나 다른 종류의 항생제로 적어도 10일 간 치료하는 것이 보통이다.
류마티스 열의 예방 Prevention of rheumatic fever
- 류마티스 열을 류마티스 열, 류머티스 열, 또는 류머트성 열이라고도 한다.
- A군 베타 용혈성 연쇄상구균 중 특별 세균종 감염에 의해 생긴 인두염이나 편도염, 또는 인두 편도염을 앓을 때 조기에 적절히 치료해서 류마티스 열을 예방해야 한다.
- 과거에 류마티스 열을 한 번 앓았던 병력이 있는 아이가 A군 베타 용혈성 연쇄상구균 감염에 의한 감염병을 앓을 때는 류마티스 열을 앓은 병력이 없는 다른 아이들보다 류마티스 열이 재발될 가능성이 10배 더 높다.
- 류마티스 열이 재 유발될 때는 류마티스 심장염이 발생될 가능성이 아주 높다.
- 과거에 류마티스 열을 한 번 앓았던 병력이 있는 아이들은 한 달에 한 번 벤자진 페니실린(Benzathine penicillin) 주사로 A군 베타 용혈성 연쇄상구균 감염병을 예방하든지,
- 경구용 페니실린을 하루에 1회 복용해서 류마티스 열이 재발되지 않도록 예방 할 수 있다. 페니실린에 알레르기가 있으면 간트린신이나 에리스로마이신 등 항생제로 예방 한다.
- 첫 류마티스 열을 앓은 이후부터 성인이 된 후에도 류마티스 열이 재발되지 않도록 페니실린이나 다른 종류의 적절한 항생제로 예방 한다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제7권 소아청소년 감염병- A군 베타 용혈성 연쇄상구균에 의한 감염병 참조).
표 3. 급성 류마티스 열을 앓았던 아이에게 류마티스 열이 발생 앓게 예방하는 방법
| 앓았던 류마티스성 열의 종류 | 예방치료하는 기간 | 급성 류마티스성 열의 재발 예방적 치료에 쓰는 항생제의 종류, 용량, 투여 경로 |
| 류마티스성 심장염이 없이 앓았던 류마티스성 열 | 5년간 또는 21세가 될 때까지 |
또는
또는
또는
또는
|
| 류마티스성 열을 앓을 때 류마티스성 심장염이 있었으나 그로 인한 후유 병변이 심장병이 생기지도 않고 심장 판막 이상이 없는 경우 | 10년 동안 또는 성인이 될 때까지 | 이상과 동일 |
| 류마티스성 열을 앓을 때 류마티스성 심장염이 있었고 그로 인한 후유 병변이 심장병에 생기고 심장 판막 이상도 있는 경우 | 적어도 마지막 류마티스성 열을 앓은 후 10년간, 또는 40세가 될 때까지, 또는 일생동안 | 이상과 동일 |
| 소스; Red book, 27th Edition, 2005. p.619
|
Rheumatic fever 류마티스 열(류머티스 열)
Overview of rheumatic fever (rheumatic fever)
• Tonsillitis, pharyngitis, pharyngeal tonsillitis, otitis media, or scarlet fever caused by group A streptococcal infection, or after recovery, an adverse reaction with the group A streptococcal antigen antibody can occur in various organs of the body, such as the connective tissue or heart. Inflammation is called rheumatic fever, rheumatic fever or rheumatic fever.
• Group A beta-hemolytic streptococci are also referred to herein as group A streptococci for convenience.
Causes of rheumatic fever (rheumatic fever)
• Group A Streptococcus When acute tonsillitis, pharyngeal tonsillitis, pharyngitis, or various other group A streptococcal infectious diseases are present in any part of the body, the connective tissue is inflamed due to an adverse reaction with the group A streptococcal antigen antibody, resulting in rheumatic fever.
• It is common to have an infectious disease caused by a group A streptococcal infection in some part of the body just before or at the time of the onset of rheumatic fever.
• Rarely, there is no recent history of infectious disease caused by group A streptococcus, and it is possible that you do not have group A streptococcal disease at the time of rheumatic fever.
www.drleepediatrics.com-Vol. See also Infectious diseases in children and adolescents – Infectious diseases caused by group A streptococcus, Respiratory diseases in children and adolescents – pharyngitis, tonsillitis, pharyngeal tonsillitis. Symptoms of rheumatic fever (rheumatic fever)
Photo 77. Group A beta-hemolytic streptococcal tonsillitis Rheumatic fever may occur when you have pharyngitis or tonsillopharyngitis. Copyright ⓒ 2013 John Sangwon Lee, MD., FAAP
• Symptoms and signs vary greatly depending on the main symptom (comorbid disease) of rheumatic fever, the progression of rheumatic fever, the presence of complications, and the type of infectious disease caused by group A streptococcus infection.
o When you have rheumatic fever
o rheumatoid carditis, o rheumatoid arthritis,
o rheumatic skin rash;
o erythema migratory (erythema marginal), o rheumatoid chorea,
o Rheumatoid nodules (subcutaneous nodules);
o Main comorbidities such as rheumatoid pneumonia may occur.
• The aforementioned rheumatic carditis, rheumatoid arthritis, rheumatoid skin rash (erythema migratory), rheumatoid chorea, and rheumatic nodules are referred to as the main comorbidities of rheumatic fever or main symptoms of rheumatic fever.
• When afflicted with rheumatic fever, not all of these major comorbidities appear at once.
• One of the main comorbidities or several or almost all of the main comorbidities of rheumatic fever may be present.
• Rheumatic fever is more common in winter and spring, when pharyngitis, tonsillitis, pharyngeal tonsillitis, and scarlet fever caused by group A streptococcal infection are more likely to occur.
• There are several strains of group A streptococci, one of which causes rheumatic fever.
• Infants before 3 years of age, infants after 3 years of age, school-age children, adolescents, and adults can also get rheumatic fever, but children aged 5 to 15 years are more likely to get rheumatic fever.
• Children living in poorly sanitary conditions and young people living in small living quarters are also more susceptible to the disease.
• Rheumatic fever can occur in 3% of children with group A streptococcal infection, but it may occur more intensively depending on a certain time and place.
• So the overall incidence of rheumatic fever is said to be only 0.3%.
• Most commonly, one or more than one of the main comorbidities of rheumatic fever develops about 1 to 5 weeks after suffering an infectious disease caused by group A streptococcus infection.
• However, rheumatoid chorea can occur even after 2 to 6 months have passed after an infectious disease caused by a group A streptococcal infection.
• Symptoms caused by pharyngitis or tonsillitis caused by group A streptococcal infection and symptoms caused by rheumatic fever may appear together.
• Also, when you have rheumatic fever, the symptoms are different depending on what kind of main comorbidity you have.
• Symptoms and signs of rheumatoid arthritis, rheumatoid chorea, rheumatoid carditis, and rheumatoid nodules may appear simultaneously.
• When you have rheumatic fever, you may experience abdominal pain similar to the symptoms of appendicitis, and you may also experience symptoms such as low fever or high fever.
• These symptoms are usually acute, but sometimes gradually become chronic.
• Each comorbidity of rheumatic fever is explained in more detail in each of the following sections.
1. Rheumatic carditis
Figure 78. With rheumatoid carditis You should take physical and mental stability as directed by your doctor. Copyright ⓒ 2011 John Sangwon Lee, M.D.. FAAP
• About 40% of children and adolescents who develop rheumatic fever for the first time can develop rheumatic carditis, one of the main comorbidities of rheumatic fever.
• In some cases, there is no other major comorbidity of rheumatic fever, but only rheumatic carditis.
• Group A beta-hemolytic streptococci are referred to as group A streptococci for convenience.
• After suffering from group A streptococcal pharyngitis and other major symptoms of rheumatoid arthritis or rheumatic fever, rheumatoid carditis may appear after 1 to 2 days of illness.
• Rheumatic carditis is one of the main comorbidities of rheumatic fever.
• With rheumatoid carditis, the lining of the heart and heart muscle are damaged. Therefore, rheumatoid endocarditis may also occur.
• Occlusion of the mitral valve between the left atrium and left ventricle or the aortic valve between the left ventricle and the aorta, or mitral or aortic valve insufficiency may occur.
• Fluid can pool in the pericardial cavity that surrounds the heart. When the disease is mild, there may be few symptoms. You may not even know you have this disease.
• In mild cases of rheumatoid carditis, there may be only irritable symptomatic signs, accompanied by weight loss and loss of appetite.
• In severe cases of rheumatic carditis, the heart enlarges abnormally, and endocarditis and heart failure can occur.
• The heart is beating fast and abnormal heart murmurs may be heard.
• If not treated early and properly, rheumatoid carditis can last for weeks to months. • After months or years of rheumatoid carditis, the heart’s mitral and aortic valves may harden, narrow, and shrink.
• The mitral and aortic valves may become abnormally narrow and small. • At this time, you may have very shortness of breath, your left breast may be pounding, and your heart may be beating rapidly.
• When rheumatoid carditis becomes severe, congestive heart failure occurs in which blood and fluid accumulate in the lungs instead of normally filled with air, causing frequent coughing and shortness of breath.
• If the heart disease continues to progress, it can be life-threatening.
2. Rheumatic arthritis
Photo 79. Severe group A beta-hemolytic streptococcal pharyngitis and tonsillitis. Swelling and red tonsils are jammed. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 80. Severe group A beta-hemolytic streptococcal pharyngitis and tonsillitis. Swelling and red tonsils are jammed. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Figure 81. Normal electrocardiogram. An electrocardiogram is done to check for any abnormalities in the heart. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 82. Chest X-ray A chest x-ray is done to check for heart problems. a – lungs, b – heart, c – diaphragm, d – trachea. Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
• About 75% of children with rheumatic fever have rheumatoid arthritis, a major comorbidity of rheumatic fever.
• Sometimes, when you have rheumatoid arthritis, your joints don’t swell significantly and you only have joint pain.
• Rheumatoid arthritis can occur simultaneously in one, two, or more joints among relatively large joints, such as the elbow joint, wrist joint, ankle joint, and knee joint. • With this disease, the joints may suddenly become red and swollen and warm. A characteristic feature of rheumatoid arthritis is that even a slight movement or gentle touch of the joint causes severe pain.
• Rheumatoid arthritis can also rarely occur in the hand joints in the hands or in the neck and hip joints in the feet.
• When you have rheumatoid arthritis, several joints may be sore but not swollen at the same time, and several joints may be swollen and painful at the same time.
• Rheumatoid arthritis may occur in one joint, causing sudden swelling and severe pain, and then all of the symptoms of arthritis may disappear suddenly, as if it all went away after a while.
• Migratory polyrheumatoid arthritis, in which arthritis with almost similar symptoms and signs moves to another joint, may also occur.
• If rheumatoid arthritis is properly treated, it is one of the characteristics of this disease that it does not leave any sequelae in the arthritis joint.
3. Rheumatic nodules
Photo 83. Upper-A blood agar culture medium covered with pharyngeal mucus before being put into the incubator for bacterial culture of group A beta-hemolytic streptococci, lower left-Bacterial blood agar culture medium grown with pharyngeal microbes that are not group A streptococci, H right-A Bacterial blood agar culture medium grown with group beta-hemolytic streptococci (group A streptococci)
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 84. Bacterial blood culture medium grown with pharyngeal microbes in the upper-bacterial culture incubator, Bacterial blood agar culture medium grown with group A streptococci Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 85. A group A streptococcal antigen-antibody aggregation test was negative Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 86. A positive group A streptococcal antigen-antibody aggregation test Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
• When you have rheumatic fever, a lump of hard connective tissue that forms in the subcutaneous tissue at the joint site is called a rheumatic subcutaneous nodule or rheumatic nodule.
• Rheumatoid nodules are one of the main comorbidities of rheumatic fever.
• Rheumatoid nodules are the size of a grain of rice or the size of a soybean bean. • It is usually not painful to touch.
• Rheumatoid nodules are more likely to develop when rheumatoid arthritis recurs or when rheumatoid carditis is more severe.
• Although rheumatic nodules themselves do not cause further health problems, they can be seen as a sign that the patient is suffering from more severe rheumatic fever.
• The presence or absence of rheumatic nodules during rheumatic fever is of clinical importance.
• Rheumatoid nodules appear in 5-10% of children with rheumatic fever.
• These rheumatic nodules usually appear several weeks after the onset of rheumatic fever.
4. Rheumatic erythema marginatum
Photo 87. Erythema migratory (erythema flexible, erythema marginal) This picture is a migratory erythema of Lyme disease. Copyright ⓒ 2011 John sangwon Lee, M.D.. FAAP
• About 5-10% of children with rheumatic fever may develop rheumatoid erythema. Erythema migratory rheumatica is called erythema migratory or marginal erythema. • Rheumatoid erythematosus is one of the main comorbidities of rheumatic fever.
• Skin rashes similar to those of rheumatoid erythematosus may appear in other conditions, such as Lyme disease.
• The appearance of this rash is helpful in diagnosing rheumatic fever, but has little to do with its severity.
• The rheumatoid erythematosus is a little red, slightly swollen, but not itchy. The edge of the rash is curved like a wave, rather distinct and rounded.
• This rash may appear more frequently on the trunk and limbs and tends to come and go and reappear.
5. Rheumatic Chorea
• Chorea is one of the main comorbidities of rheumatic fever.
• Chorea is also called rheumatic chorea.
• If you have rheumatoid chorea, you may move one or both faces, arms, etc., without purpose, in rhythmic and out-of-order dance movements.
• Chorea may appear together with the other main symptoms of rheumatic fever, or it may appear separately.
• When symptoms of chorea appear, they suddenly move like dancing, and at that time they cannot consciously control their body, which can injure themselves.
• There may be difficulties in writing or speaking, and emotional abnormalities may appear suddenly due to emotional instability.
• Without proper treatment, it can last for weeks, months, or even a year.
6. Rheumatic pneumonia
• When you have rheumatic fever, you may have comorbidities such as rheumatic pneumonia.
• Rheumatoid pneumonia is not an infectious disease caused by a direct infection of the lungs with pathogens such as bacteria or viruses, but pneumonia caused by an adverse reaction with the group A beta-hemolytic streptococcal antigen antibody.
Diagnosis of rheumatic fever
• Rheumatic fever is not a disease that is cured once, but can be re-induced after it is cured, so preventative treatment should be continued. It is important to confirm the diagnosis
• Since rheumatic fever can recur, it is essential to prevent recurrence of rheumatic fever. It is necessary to accurately diagnose rheumatic pneumonia from the beginning and also diagnose and treat rheumatic fever.
• Prevent recurrence of rheumatic fever and rheumatic pneumonia.
• If rheumatic fever is suspected based on the medical history, symptom signs, and examination findings, it is common to be hospitalized for diagnostic treatment.
• Diagnosis is made by performing a group A beta-hemolytic streptococcal bacterial culture test or a group A beta-hemolytic streptococcal antigen antibody agglutination test with a mucus specimen collected from the pharyngeal tonsil mucosal layer.
o Other ASO blood tests;
o ESR test; o ECG,
o CPR tests;
o chest x-ray,
o Diagnosis by echocardiography and other appropriate tests.
• Aspirin is particularly effective in treating rheumatic fever. However, if you are not sure if you have rheumatic fever and you are treated with aspirin, the symptoms of rheumatic fever may improve quickly, but it will interfere with the early diagnosis of rheumatic fever.
• The disease seems to get better, but if prevention is neglected, it may recur.
• Do not take anti-inflammatory or antipyretic drugs such as aspirin without a doctor’s diagnosis and prescription to determine whether arthritis, heart disease, or other diseases are caused by rheumatic fever.
• Treatment differs depending on the course of rheumatic fever and the severity of comorbidities.
www.drleepediatrics.com-Volume 11 Children and Adolescent Cardiovascular Diseases-Refer to rheumatic fever. Gentral treatment of rheumatic fever
1. Take mental and physical stability.
• Diagnosis and treatment differ depending on the severity, progression, and age of the main comorbidities of rheumatic fever.
• Depending on the severity of rheumatoid carditis, mental and physical stability is an important treatment
• When you are seriously ill, you should be physically stable so that you can urinate indoors and eat food in bed.
• When you have rheumatic heart disease, it is very important to rest mentally and physically for 3 weeks to 3 months.
• If you suffer from rheumatic fever without rheumatic carditis, one of the main comorbidities of rheumatic fever, you may begin to do physical maneuvers gradually when the severity improves 7 to 10 days after starting treatment and your mood and energy improve.
2. Treat with aspirin according to your doctor’s prescription.
• Rheumatic fever can be treated with aspirin, and if necessary, two drugs, aspirin and prednisone.
• When treating rheumatic fever, the therapeutic dose of aspirin is much higher than the therapeutic dose of aspirin when other diseases are treated with aspirin.
• When treated with aspirin, tinnitus, gastrointestinal disturbances, and various other side effects and adverse drug reactions may occur.
• After at least 10 days of treatment with aspirin, aspirin treatment is no longer necessary when the severity improves.
• Treatment with prednisone can also cause many side effects, and treatment is generally performed for 4 to 6 weeks.
3. Rheumatic fever can occur during or after pharyngitis and tonsillitis caused by group A beta-hemolytic streptococci.
• First, it is necessary to check for infectious diseases caused by group A beta-hemolytic streptococcus infection.
• Group A beta-hemolytic streptococcus culture test can be performed with a mucus specimen obtained from an infectious disease lesion in the pharynx or other parts of the body, and rheumatic fever can be diagnosed based on the results.
• If you have rheumatic fever, even if group A beta-hemolytic streptococcus is not cultured in the bacterial culture, it is usually treated with penicillin or other antibiotics for at least 10 days.
Prevention of rheumatic fever
• Rheumatic fever is also called rheumatic fever, rheumatic fever, or rheumatic fever.
• In case of pharyngitis, tonsillitis, or pharyngeal tonsillitis caused by infection with a special bacterial species of group A beta-hemolytic streptococci, early and appropriate treatment should be used to prevent rheumatic fever.
• Children with a previous history of rheumatic fever are 10 times more likely to have a recurrence of rheumatic fever when they have an infection caused by a group A beta-hemolytic streptococcal infection than other children without a history of rheumatic fever.
• When rheumatic fever recurs, the likelihood of developing rheumatic carditis is very high.
• For children with a history of one past rheumatic fever, administer Benzathine penicillin once a month to prevent group A beta-hemolytic streptococcal infection;
• Taking oral penicillin once a day can prevent recurrence of rheumatic fever. If you are allergic to penicillin, prevent it with antibiotics such as gantrisin or erythromycin. • Prevent recurrence of rheumatic fever from the first rheumatic fever into adulthood with penicillin or other appropriate antibiotics. www.drleepediatrics.com
– Volume 7 Infectious Diseases in Children and Adolescents – See Infectious Diseases Caused by Group A Beta Hemolytic Streptococcus).
Table 3. How to prevent rheumatic fever in a child who has had acute rheumatic fever 표 3. 급성 류마티스 열을 앓았던 아이에게 류마티스 열이 발생 앓게 예방하는 방법
| Types of rheumatic fever you suffered from |
period of prophylaxis
|
Types, doses, and routes of administration of antibiotics used for prophylactic treatment of acute rheumatic fever |
| Rheumatic fever without rheumatic carditis | 5 years or until age 21 |
|
| When you had rheumatic fever, you had rheumatic carditis, but the sequelae lesion did not cause heart disease and there was no heart valve abnormality. | for 10 years or until adulthood | same as above |
| When you had rheumatic fever, you had rheumatic carditis, and the sequelae lesion caused by heart disease and heart valve abnormalities | At least 10 years after the last rheumatic fever, or until the age of 40, or for the rest of your life. | same as above |
| sources; Red book, 27th Edition, 2005. p.619
|
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community,American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”