로타바이러스 위장염(로타바이러스성 위장염), Rotavirus gastroenteritis(Rotavirus infection/Rotaviral gastroenteritis)
(You may visit www.drleepediatrics.com – Volume 7,
Pediatric Adolescent Infectious Diseases or제 7권, 소아 청소년 감염병 질환 웹사이트)
로타바이러스 위장염(로타바이러스성 위장염)의 원인
- 로타바이러스 감염(Rotavirus infection)으로 생긴 바이러스성 위장염을 로타바이러스 위장염(Rotavirus gastroenteritis), 또는 로타바이러스성 위장염(Rotaviral gastroenteritis)이라 한다.
- 로타바이러스 위장염은 어느 연령층 아이들에게도 생길 수 있지만 생후 6개월부터 2세까지 영유아들에게 더 잘 생긴다.
- 로타바이러스 위장염은 여러 종류의 급성 위장염들 중 가장 흔한 위장염이다.
- 로타바이러스성 위장염을 앓는 환자의 대소변으로 나온 로타바이러스에 오염된 음식물을 먹거나 대소변 속에서 나온 로타바이러스가 묻은 변기 등을 만진 불결한 손으로 음식물을 먹을 때 로타바이러스가 경구를 통해 위장관으로 감염되는 경우가 가장 흔한 감염경로이다.
- 로타바이러스 위장염은 세계 각처 어느 나라에서도 발생된다.
- 그렇지만 비위생적이고 밀접한 거주환경에서 사는 아이들에게 이 병이 더 잘 발생될 수 있다.
- 이 병은 사시사철 어느 계절에도 유행될 수 있으나 1~4월에 더 많이 유행되며 로타바이러스 감염성이 매우 강하다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제9권 소아청소년 소화기 질환-로타바이러스로 인한 위장염 참조.
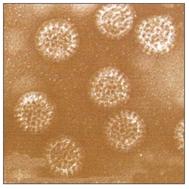
사진 3-77. 전자 현미경으로 본 로타바이러스 사진.출처-CDC
로타바이러스 위장염(로타바이러스성 위장염)의 증상 징후
| 병일증상 | -4 | -3 | -2 | -1 | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||||
| 설 사 | 감염 | |||||||||||||||||||
| 열 | ||||||||||||||||||||
| 구토 | ||||||||||||||||||||
| 바이러스 전파 | ||||||||||||||||||||
그림 3-78. 병일에 따른 전형적 로타바이스 위장염 증상 징후
출처-Pediatric annals July 2006
- 증상 징후는 다양하고 나이, 정도, 탈수의 정도, 합병증의 유무 등에 따라 다르다.
- 로타바이러스가 인체에 감염되어 아무 증상 징후가 없이 면역체만 남길 수 있고, 설사, 탈수 등 여러 증상 징후가 심하게 생길 수도 있다.
- 로타바이러스 위장염의 전형적인 증상 징후는 다음과 같다.
- 미열 내지 고열이 나고, 갑자기 구토하면서 며칠간 심하게 물 설사를 할 수 있다.
- 구토 설사로 심하게 탈수 될 수 있다.
- 설사 변의 색은 황색, 녹색, 때로는 쌀뜨물 색이다.
- 먹는 음식물의 색에 따라 설사변의 색이 다양할 수 있다.
- 곱이나 피가 섞여 있지 않은 것이 보통이다.
- 복통이 생길 수 있다.
- 음식물을 제대로 먹을 수 없고 구토 설사로 쉽게 탈수 될 수 있다.
- 1~2일 동안만 설사를 할 수도 있고 15일 정도 오랫동안 계속 설사 할 수 있다.
- 일반적으로 나이가 어리면 어릴수록, 열이 나고 구토 설사를 하면서 더 쉽게 탈수된다.
- 때문에 영유아들이 로타바이러스 위장염에 걸리면 영유아기 이후 아이들에 비해 더 심하게 빨리 탈수된다. 그래서 탈수와 전해질 불균형증과 산혈증이 동시 생길 수 있다.
- 잠복기는 약 1~3일이다.
로타바이러스 위장염(로타바이러스성 위장염)의 진단
- 병력, 증상 징후, 진찰소견을 종합하여 이 병을 진단하는 것이 보통이다.
- 같은 동네에서 일부 아이들이 로타바이러스 위장염을 앓고 있을 때 그 동네 다른 아이들도 로타바이러스 위장염의 증상 징후와 비슷한 설사와 구토 등으로 앓으면, 아마도 이 아이도 로타바이러스 위장염에 걸렸다고 추정 진단 할 수 있다.
- 환아의 대소변으로 효소면역 검정법, 엘리사 검사, 또는 CF 검사 등으로 확진할 수 있다.
로타바이러스 위장염(로타바이러스성 위장염)의 치료
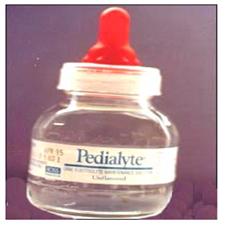
사진 3-79. 페디아라이트 등 경구용 포도당 전해질 용액으로 로타바이러스 위장염으로 생긴 설사 구토로 생긴 탈수를 예방적 치료를 한다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- 증상 징후의 정도, 합병증의 유무 등에 따라 경구용 또는 정맥 주사용 포도당 전해질 용액 재수화 치료, 현상유지 수화치료, 음식물 조절 등으로 대증 치료를 한다.
- 특히 열, 복통, 구토, 설사 등으로 탈수가 심하게 생겼을 때는 병원에 입원하여 재수화 치료하는 것이 보통이다. 병원에서는 경구 포도당 수분 전해질 공급 치료도 하고 필요에 따라 정맥 포도당 수분 전해질 공급치료도 하고 열은 해열제로 치료한다.
- 때로는 맹물만 조금 마셔도 토하고 설사를 심하게 해서 계속 탈수되고 탈진될 수 있다.
- 이럴 때는 병원에서 포도당 전해질용액 정맥 혈관주사로 수분 전해질 공급치료를 한다.
- 구토나 설사를 경하게 할 때는 집에서 의사의 지시에 따라 페디아라이트 액 등 경구용 포도당 전해질용액을 경구로 먹여 재수화 치료 및 현상유지 수화 치료를 시작할 수 있다.
- 로타바이러스 위장염의 증상 징후가 점차로 더 좋아질 때는 처음 얼마 동안 주었던 페디아라이트 액 등 포도당 전해질용액의 양을 점차로 늘려줄 수 있다.
- 중증도가 점차로 더 좋아지는 시점에서 페디아라이트 액의 양을 줄려 주기 시작하면서 전 유동음식물을 주기 시작한다.
- 전 유동음식물을 몇 번 먹고 구토와 설사의 증상 징후가 덜 해지고 탈수치료의 경과가 계속 더 좋아지면 페디아라이트 액을 더 이상 주지 않을 수 있다.
- 그 다음은 전 유동 음식물의 양을 점점 늘려 주다가 병의 경과가 점점 더 좋아지면 그 다음에는 전 유동 음식물에서 반 유동 음식물로, 그 다음에는 반 유동 음식물에서 보통 때 먹었던 음식물로 서서히 1~2일 거쳐 바꾸어 줄 수 있다.
- 이런 치료는 어디까지나 단골 소아청소년과 의사의 지시에 따라 하는 것이 원칙이다.
- 모유를 먹는 영유아들이 로타바이러스 위장염으로 설사를 할 때는 구토를 하지 않으면, 또는 모유를 계속 먹을 수 없을 때를 제외하고는 모유를 계속 먹을 수 있다.
- 이런저런 치료도 어디까지나 그때 상황에 따라 의사의 지시에 따라 치료하는 것이 치료 원칙이다.
- 항생제는 이 병에 효력이 없다.
- 대부분의 “설사치료 약”이나 “위장 치료 약”도 별 효과가 없다.
- 공생세균제(Probiotics)에 치료 효과가 있다는 연구결과도 있다. 그 치료에 관해서 찬반이 있다.
- 로타바이러스 위장염으로 영유아가 구토와 설사를 조금 할 때는 의사의 지시에 따라 경구용 포도당 전해질용액으로 치료하는 것이 보통이다.
- 적어도 첫 2~4시간 동안 페디아라이트 등 경구용 포도당 전해질 용액으로 탈수치료 재수화 치료를 의사의 지시에 따라 하든지 모유만 먹이고 다른 음식물을 일절 주지 말고 관찰 치료를 할 수 있다. 그 다음 구토를 하지 않으면 페디아라이트 액 등의 경구용 포도당 전해질 용액 30~120cc 정도를 2~3시간마다 먹여 탈수치료, 재수화 치료를 하든지 모유를 계속 먹일 수 있다. 이 때도 역시 의사의 지시에 따라 치료한다.
- 이렇게 치료하는 동안 설사나 구토를 조금씩 하든지 거의 하지 않으면 그 다음 12~24시간 동안 페디아라이트 액 등의 경구용 포도당 전해질용액을 계속 더 주어 예방적 탈수 치료한다. 경구용 포도당 전해질용액의 용량과 얼마나 오랫동안 주어야 하는지는 아이의 나이, 체중, 증상 중증도 등에 따라 의사와 상의해서 결정한다.
- 이상은 치료 예는 경도로 설사하고 경도로 탈수증을 가진 영유아들의 로타바이러스 위장염을 치료하는 예이다.
- 로타바이러스 위장염을 앓을 때 우유나 우유가 섞인 음식물을 먹으면 설사를 더 심하게 할 수 있다. 그리고 설사나 위장염으로 다른 증상 징후가 더 이상 생기지 않은 마지막 날로부터 3~5일 동안 우유나 우유가 섞인 음식물을 먹여서는 안 된다.
- 페디아라이트 액이나 다른 종류의 경구용 포도당 전해질 용액을 먹이는 대신 보리차나 맹물을 조금씩 줄 수 있으나 보리차나 맹물에는 전해질 성분도 포도당 성분이 거의 들어 있지 않기 때문에 보리차나 맹물을 많이 먹으면 더 탈수될 수 있고 혈중 전해질 불균형이 생길 수 있다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제1권 소아청소년 응급의료-급성 탈수증, 설사와 구토로 인한 탈수증, 설사 및 구토의 일반적인 치료, 제9권 소아청소년 소화기 질병 참조.
로타바이러스 위장염(로타바이러스성 위장염) 환자의 격리
- 이 병을 앓는 환아는 집안 식구들로부터 격리시킬 필요는 없다.
- 병원 입원치료를 할 때는 다른 사람들로부터 환아를 격리시키고 치료한다.
환자와 접촉한 경우
- 이 병이 유행될 때나, 이 병을 앓는 환아와 접촉했을 때는 보통 때보다 손을 더 깨끗이 씻고 그 외 다른 위생 관리를 더 철저히 해서 이 병을 예방한다.
- 사람들이 많이 모인 곳에 영유아들을 데리고 가서는 안 된다.
- 특히 이 병이 유행될 때는 더 그렇다.
표 3-4. 로타바이러스 감염병 백신 예방접종
| 백신의 종류접종 받는 조건 | 로타릭스 백신 Rotarix Vaccine | 로타테크 백신 Rota-Teq Vaccine |
| 예방접종 횟수 | 2회 | 3회 |
| 예방접종 연령 | 생후 2, 4개월 | 생후 2, 4, 6개월 |
| 최초 예방접종을 받을 수 있는 최초 연령 | 생후 6주 | |
| 최초 예방접종을 받을 수 있는 최후 연령 | 생후13개월(특별히 13주 6일) | |
| 각 예방접종 간격 | 4주나 그 이상 | |
| 최종 예방접종을 해 줄 수 있는 최후 연령 | 생후 32주(특별히 32주 6일) | |
출처; Infectious disease in children, April 2008, p.14
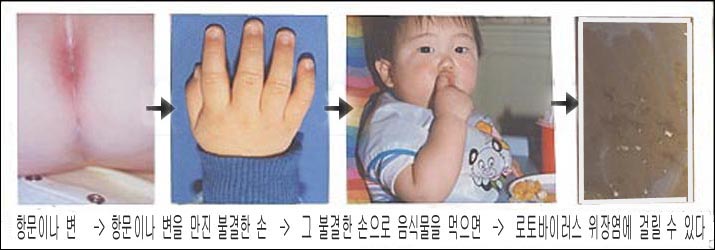
사진 3-80. 로타바이러스 위장염에 걸리는 감염 경로
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
- 1998년에 로타쉴드(Rotashield) 예방접종 백신이 개발되어 로타쉴드 백신으로 로타바이러스 감염성 위장염을 예방접종했었다. 그러나 로타쉴드 백신으로 예방접종 받은 소아들 50,000~100,000명 중 1명꼴로 장중적증이 발생됐다. 1999년 이후부터 로타쉴드 백신 예방접종을 더 이상 권장하지 않았다.
- 그 후 새로운 연구결과로 2006년 2월에 로타바이러스 위장염 예방접종 백신 “Rota-Teq Vaccine”이 새로 개발되어 미 FDA에 의해 허가됐다.
- Rota-Teq 백신을 생후 2, 4, 6개월에 1차, 2차, 3차 접종, 총 3차 접종해서 로타바이러스 감염성 위장염을 예방해 주는 것을 권장하고 로타바이러스 백신을 모든 영아들이 접종받아야하는 기본 예방접종이다.
- 생후 2, 4, 6개월에 각각 1차, 2차, 3차, 총 3차 접종을 다 받지 못했을 때는 1차 Rota Teq 백신은 적어도 생후 6~12개월에 접종 받고, 그 다음 2차 예방접종은 1차 접종을 받은 후 6~12주 간격을 두고 접종 받고 3차 접종은 적어도 생후 32주 이전에 접종받으라고 권장한다.
- Rota Teq 백신으로 예방접종을 받았을 때 예방접종 효과는 거의 100 %이라고 한다.
- 열이 경미하게 나거나 모유를 먹는 영유아도 Rota-Teq 백신으로 접종받을 수 있다고 한다.
- 표 3-4에서 설명한 것 같이 최근 로타릭스(Rotarix vaccine) 백신이 또 나왔다.
- 그 예방접종 방법은 그 표에서 참조한다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제9권 소아청소년 소화기 질환-로타바이러스성 위장염 참조.
Rotavirus gastroenteritis (Rotavirus infection/Rotaviral gastroenteritis) 로타바이러스 위장염(로타바이러스성 위장염)
Causes of rotavirus gastroenteritis (rotaviral gastroenteritis)
• Viral gastroenteritis caused by rotavirus infection is called Rotavirus gastroenteritis, or Rotaviral gastroenteritis. • Rotavirus gastroenteritis can occur in children of any age, but it is more common in infants and young children from 6 months to 2 years of age.
• Rotavirus gastroenteritis is the most common of several types of acute gastroenteritis.
• Rotavirus is infected orally into the gastrointestinal tract when eating food contaminated with rotavirus from the feces of a patient with rotaviral gastroenteritis, or eating food with dirty hands that have touched a toilet with rotavirus from the stool. Is the most common route of infection.
• Rotavirus gastroenteritis occurs in any country in the world.
• Nevertheless, the disease may be more prevalent in children who live in unsanitary and close-dwelling environments.
• The disease can spread in any season of the year, but it is more prevalent in January to April and is highly infectious to rotavirus. www.drleepediatrics.com-Volume 9 Children and Adolescents Digestive Diseases-Refer to the gastroenteritis caused by rotavirus.
Photo 3-77. Rotavirus photo seen under an electron microscope. Source-CDC
Symptoms signs of rotavirus gastroenteritis (rotaviral gastroenteritis)
| sick day/symptom | -4 | -3 | -2 | -1 | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||||
| diarrhea | infectious | |||||||||||||||||||
| fever | ||||||||||||||||||||
| vomiting | ||||||||||||||||||||
| Virus spreading | ||||||||||||||||||||
Figure 3-78. Typical symptoms of rotavirus gastroenteritis depending on the illness Source-Pediatric annals July 2006
• Symptoms and signs vary and depend on age, severity, degree of dehydration, and the presence or absence of complications.
• Rotavirus can infect the human body, leaving only the immune system without any symptoms, and various symptoms such as diarrhea and dehydration can be severe.
• Typical symptomatic signs of rotavirus gastroenteritis are:
• You may have a mild to high fever, vomiting suddenly, and have severe watery diarrhea for several days.
• Vomiting and diarrhea can lead to severe dehydration.
• Diarrhea The color of the stool is yellow, green, and sometimes rice water.
• The color of diarrhea may vary depending on the color of the food you eat. • It is usually not mixed with blood or blood.
• You may have abdominal pain.
• You cannot eat properly and can easily become dehydrated from vomiting and diarrhea.
• You may have diarrhea only for 1 to 2 days, or you may have diarrhea for as long as 15 days.
• In general, the younger you are, the more easily you become dehydrated with fever and vomiting and diarrhea.
• Because of this, when infants and toddlers get rotavirus gastroenteritis, they become dehydrated more rapidly than children after infancy. So, dehydration, electrolyte imbalance, and acidemia can occur at the same time.
• The incubation period is about 1 to 3 days. Diagnosis of rotavirus gastroenteritis (rotaviral gastroenteritis)
• It is common to diagnose this disease by combining the medical history, symptoms, and examination findings.
• If some children in the same neighborhood have rotavirus gastroenteritis, and other children in that neighborhood also suffer from diarrhea and vomiting similar to symptoms of rotavirus gastroenteritis, the child may be presumably diagnosed with rotavirus gastroenteritis.
• The feces of a patient can be confirmed by enzyme immunity test, ELISA test, or CF test.
Treatment of rotavirus gastroenteritis (rotaviral gastroenteritis)
Photo 3-79. Prophylactic treatment of dehydration caused by diarrhea and vomiting caused by rotavirus gastroenteritis is performed with oral glucose electrolyte solutions such as Pedialite. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• Depending on the severity of symptoms and the presence or absence of complications, symptomatic treatment is provided through oral or intravenous glucose electrolyte solution rehydration treatment, status maintenance hydration treatment, and food control.
• In particular, when dehydration is severe due to fever, abdominal pain, vomiting, or diarrhea, it is common to be admitted to a hospital for rehydration treatment. In hospitals, oral glucose water-electrolyte supply treatment is provided, intravenous glucose water-electrolyte supply treatment is provided, and fever is treated with antipyretic drugs.
• Sometimes drinking a small amount of plain water can lead to vomiting and severe diarrhea, resulting in continued dehydration and exhaustion.
• In this case, hydration electrolyte supply treatment is performed by intravenous vascular injection of glucose electrolyte solution at the hospital.
• When vomiting or diarrhea is mild, rehydration treatment and status maintenance hydration treatment can be started by feeding oral glucose electrolyte solutions such as Pedialyte solution orally according to the doctor’s instructions at home.
• When symptoms of rotavirus gastroenteritis are gradually getting better, the amount of glucose electrolyte solution, such as Pedialyte solution given for the first time, maybe gradually increased.
• At the point where the severity gets better, the amount of Pedialite liquid begins to decrease and the whole fluid begins to be dispensed.
• If you have eaten a few liquid foods before, and the symptoms of vomiting and diarrhea are less, and the course of dehydration continues to improve, you may not give Pedialite liquid any more.
• Then, gradually increase the amount of all-fluid food, and when the disease progresses more and more, then, from all-fluid food to semi-fluid food, and then from semi-fluid food to normal food, gradually for 1 to 2 days. You can change it through.
• In principle, such treatment should be performed according to the instructions of a regular pediatrician.
• When breastfed infants have diarrhea from rotavirus gastroenteritis, they can continue to eat breast milk unless they are vomiting or are unable to continue breastfeeding.
• The principle of treatment is to treat one or another treatment according to the doctor’s instructions depending on the situation at that time.
• Antibiotics have no effect on this disease.
• Most “diarrhea drugs” or “gastric drugs” don’t work very well.
• Some studies have shown that probiotics have therapeutic effects. There are pros and cons to the treatment.
• When infants and toddlers have a little vomiting and diarrhea due to rotavirus gastroenteritis, it is common to treat them with an oral glucose electrolyte solution as directed by a doctor.
• For at least the first 2-4 hours, you can perform dehydration treatment, rehydration treatment with an oral glucose electrolyte solution such as Pedialyte, as directed by your doctor, or you can do observational treatment without feeding only breast milk and no other food. Then, if you do not vomit, you can feed about 30 to 120 cc of an oral glucose electrolyte solution such as Pedialyte solution every 2 to 3 hours, and continue to feed breast milk for dehydration treatment or rehydration treatment. In this case, it is also treated according to the doctor’s instructions.
• If you do little or no diarrhea or vomiting during this treatment, continue to give an oral glucose electrolyte solution such as Pedialyte solution for the next 12 to 24 hours to treat prophylactic dehydration.
The dosage of the oral glucose electrolyte solution and how long it should be given is determined by consulting a doctor according to the child’s age, weight, and symptom severity. • An example of treatment is the treatment of rotavirus gastroenteritis in infants with mild diarrhea and mild dehydration.
• If you have rotavirus gastroenteritis, eating milk or foods mixed with milk can make your diarrhea worse. In addition, you should not eat milk or milk-infused foods for 3 to 5 days from the last day when diarrhea or gastroenteritis no longer causes any other symptoms.
• Instead of feeding Pedialite liquid or other types of oral glucose electrolyte solutions, barley tea or plain water can be given little by little. However, since barley tea or plain water contains almost no glucose components, eating a lot of barley tea or freshwater may lead to more dehydration and blood circulation. Electrolyte imbalance can occur.
www.drleepediatrics.com-Vol. 1 Children’s and Adolescent Emergency Medical Services-Acute dehydration, dehydration due to diarrhea and vomiting, general treatment of diarrhea and vomiting, see Vol. 9, Children’s and Adolescent Digestive Diseases.
Isolation of patients with rotavirus gastroenteritis (rotaviral gastroenteritis)
• Children with this disease do not need to be isolated from household members.
• In hospital inpatient treatment, the patient is isolated from others and treated.
In case of contact with the patient
• When the disease is epidemic or when you come into contact with a patient with the disease, wash your hands more thoroughly than usual and do other hygiene measures to prevent the disease. • Do not take infants and toddlers to places with large crowds.
• Especially when the disease is outbreaks.
Table 3-4. Rotavirus infectious disease vaccination
표 3-4. 로타바이러스 감염병 백신 예방접종
| Types of Vaccine /Conditions for Vaccination | Rotarix Vaccine | Rota-Teq Vaccine |
| Number of vaccinations | 2 doses | 3 doses |
| Vaccination age | 2 to 4 months old | , 4, 6 months old |
| The first age to receive the first vaccination | 6 weeks after birth | |
| The first age to receive the first vaccination | 13 months old (specially 13 weeks 6 days) | |
| Each vaccination interval | 4 weeks or more | |
| Last age for final vaccination |
32 weeks after birth (especially 32 weeks 6 days)
|
|
source; Infectious disease in children, April 2008, p.14
Photo 3-80. Routes of infection for rotavirus gastroenteritis Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
• In 1998, the Rotashield vaccination vaccine was developed, and rotavirus infectious gastroenteritis was vaccinated with the Rotashield vaccine. However, one out of 50,000 to 100,000 children vaccinated with the Rota Shield vaccine developed intestinal tract disease.
Since 1999, RotaShield vaccination has no longer been recommended.
• Subsequently, as a result of new research, in February 2006, the rotavirus gastroenteritis vaccination vaccine “Rota-Teq Vaccine” was newly developed and approved by the US FDA.
• Rota-Teq vaccine is recommended to prevent rotavirus infectious gastroenteritis by receiving the first, second, and third doses of the vaccine at 2, 4, and 6 months of age, and the basic that all infants should receive the rotavirus vaccine. It is vaccination.
• If you have not received all of the 1st, 2nd, 3rd, and 3rd doses at 2, 4, 6 months of age, respectively, the 1st Rota Teq vaccine should be given at least 6-12 months of age, followed by the 2nd vaccination. It is recommended to receive the vaccination every 6 to 12 weeks after receiving the first vaccination, and to receive the vaccination at least 32 weeks before the third vaccination.
• When vaccinated with the Rota Teq vaccine, the vaccination effect is said to be nearly 100%. • Infants with mild fever or breastfeeding can also be vaccinated with the Rota-Teq vaccine.
• As described in Table 3-4, another Rotarix vaccine has recently emerged.
• The vaccination method is referenced in the table. www.drleepediatrics.cpm-Volume 9 Children and Adolescents Digestive Diseases-Refer to Rotaviral Gastroenteritis.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey grant, and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
- The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
- Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Manual of Emergency Care
- 응급환자관리 정담미디어
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- Neonatal Resuscitation American heart Association
- Neonatology Jeffrey J.Pomerance, C. Joan Richardson
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
- Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
- Preparation for Birth. Beverly Savage and Dianna Smith
- Nelson Textbook of Pediatrics 14th ed. Beherman,
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
- Red book 29th edition 2012
- Nelson Text Book of Pediatrics 19th Edition
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gerhon, Catherine Wilfert
- The Harriet Lane Handbook 19th Edition
- 소아과학 대한교과서
- 제1권 소아청소년 응급의료 참조문헌과 출처
- Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”