대혈관 전위 Transposition of the great arteries
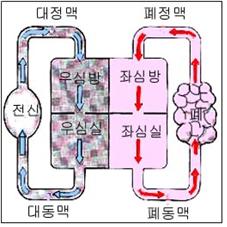
그림 51. 대혈관 전위
화살표(→)는 혈액의 흐름 방향
Copyright ⓒ 2013 John Sangwon Lee, MD., FAAP
-
대동맥은 좌심실에서, 폐동맥은 우심실에 연결되는 것이 정상인데, 반대로 대동맥이 우심실에, 폐동맥은 좌심실에 연결되는 선천성 심장 기형을 대혈관 전위 또는 폐동맥과 대동맥 전위라고 한다(그림 51 참조).
-
심방의 위치가 정위이든지 역위이고, 심방–심실의 연결에 동향성이 있고, 심실–대혈관 관계가 적합하게 되어 있지 않은 선천성 심장 기형을 대혈관 전위라고 한다.
-
대혈관 전위가 있으면 전신에서 흘러온 정맥혈이 우심방→우심실→대동맥으로 흘러간다(그림 51, 그림 3 참조).
-
대동맥으로 흘러 들어간 정맥혈이 폐를 거치지 않고 직접 전신으로 흐른다.
-
대동맥 속을 거쳐 전신으로 흘러간 피는 폐를 거치지 않은 순 정맥혈이고 그 정맥혈을 공급받은 전신에 중추성 청색증이 생긴다.
-
폐에서 흘러오는 동맥혈은 좌심방→좌심실→폐동맥→폐→폐정맥→좌심방 순서로 순환된다.
-
대정맥에서 흘러간 정맥혈은 우심방→우심실→대동맥→전신→대정맥→우심방→우심실→대동맥의 순으로 순환한다.
-
동맥혈은 폐동맥→폐 →폐정맥→좌심방→좌심실→폐동맥→폐 속으로 또다시 순환한다.
-
따라서 전신으로 흘러간 정맥혈은 폐 속으로 들어갈 기회가 전혀 없기 때문에 폐에서 산소를 공급받을 기회도 전혀 없다.
-
그래서 두 벌의 혈액순환에서 어떤 다른 선천성 심장 기형이 있어야 생존 할 수 있다.
대혈관 전위의 증상 징후
-
대혈관 전위만 가지고 태어난 신생아의 피부는 파랗다.
-
그러나 대혈관 전위가 있을 때 출생 전부터 정상적으로 가지고 있던 난원 공이 출생 이후에도 계속 열려 있거나, 좌우 심실 사이에 있는 심실 중격에 심실 중격 결손이 공존해 있거나
-
또는 그 외 다른 선천성 심장혈관 기형을 동시에 가지고 있는 경우가 많다.
-
대혈관 전위가 있을 때 난원 공이나 심방 중격 결손 또는 심실 중격 결손 등의 선천성 심장혈관 기형이 함께 있어야만 잠시 동안이라도 살 수 있다.
-
순 대 혈관 전위만 있고 다른 종류의 선천성 심장혈관 기형이 있지 않을 때는 응급 심장 수술로 임시로 좌우 심장 사이에 피가 서로 교통하도록 심장혈관 고식 치료를 응급으로 해 주지 않으면 곧 사망한다.
대혈관 전위의 진단 치료
-
병력, 증상 징후, 진찰소견 등을 종합하여 이 병이 의심되면 가슴 X-선 사진 검사, 심초음파 검사, 심전도 검사, 그 밖에 다른 검사를 응급으로 해서 진단하면서 치료를 동시한다.
-
갓 태어난 신생아에게 대 혈관 전위가 있다고 의심되면, 심장 카세터 풍선 심방 중격 절개 수술 치료로 난원 공을 더 크게 뚫어 주는 치료를 응급으로 해 준다.
-
치료할 때는 따뜻하게 보온해 주고 산소호흡 치료를 한다.
-
심장카세터 풍선 심장 중격 절개 수술 치료를 받은 후 전신이 파랗던 신생아가 핑크색 피부로 바로 변하는 치료 효과를 보면 놀라울 정도이다.
-
대혈관 전위를 가진 신생아에게 저혈당증이 잘 생길 수 있다.
-
포도당액 혈관주사로 저혈당 예방적 치료한다.
-
심장 카테터 응급치료를 해 준 후 적기에 전신에서 흘러온 정맥혈이 좌심방으로, 폐에서 흘러온 동맥혈은 우심방으로 흘러가도록, 즉 동맥혈이 대동맥을 통과해서 전신으로 흘러가게 하고 정맥혈이 폐동맥을 통과해서 폐로 들어가게 하는 고식 심장 수술치료를 해 준다.
-
그밖에 더 많은 종류의 고식수술치료방법이 있다.
Transposition of the great arteries 대혈관 전위
Figure 51. Greater vessel translocation Arrow (→) is the direction of blood flow Copyright ⓒ 2013 John Sangwon Lee, MD., FAAP
• The aorta is normally connected to the left ventricle and the pulmonary artery to the right ventricle. Conversely, the aorta is connected to the right ventricle and the pulmonary artery to the left ventricle.
• Congenital heart anomalies in which the atrial location is stereotactic or inverted, the atrial-ventricular connection is oriented, and the ventricular-large vessel relationship is not appropriate is called macrovascular translocation. • If there is a great vessel potential, venous blood from the whole body flows from the right atrium to the right ventricle to the aorta (see Fig. 51 and Fig. 3).
• Venous blood flowing into the aorta flows directly throughout the body without going through the lungs.
• The blood that flows through the aorta and into the body is pure venous blood that does not pass through the lungs, and central cyanosis occurs in the whole body receiving the venous blood. • Arterial blood flowing from the lung circulates in the order of left atrium → left ventricle → pulmonary artery → lung → pulmonary vein → left atrium.
• Venous blood flowing from the vena cava circulates in the order of right atrium → right ventricle → aorta → whole body → vena cava → right atrium → right ventricle → aorta.
• Arterial blood circulates again into the pulmonary artery → lung → pulmonary vein → left atrium → left ventricle → pulmonary artery → lung.
• Therefore, since venous blood flowing throughout the body has no chance to enter the lungs, there is no chance to receive oxygen from the lungs.
• So, you must have some other congenital heart malformation in the two sets of blood circulation to survive.
Symptoms signs of a large vessel translocation
• Newborns born with only great vessel potential have blue skin.
• However, when there is a large vessel dislocation, the ovarian ball, which was normally held before birth, remains open even after birth, or a ventricular septal defect coexists in the ventricular septum between the left and right ventricles.
• Or, they often have other congenital cardiovascular malformations at the same time.
• Congenital cardiovascular anomalies, such as oval or atrial septal defects or ventricular septal defects, must be present in the presence of large blood vessel dislocations in order to survive even for a short time.
• When there is only pure to vascular dislocation and no other types of congenital cardiovascular anomalies, emergency cardiovascular surgery temporarily dies if cardiovascular palliative treatment is not provided as an emergency so that blood flows between the left and right hearts temporarily.
Diagnosis and treatment of large vessel translocation
• If the disease is suspected by taking the medical history, symptoms, signs, and examination findings together, a chest X-ray scan, an echocardiogram, an electrocardiogram, and other tests are diagnosed as an emergency and treated simultaneously.
• If a newborn baby is suspected of having a large vascular dislocation, a cardiac catheter balloon atrial septal incision is an emergency treatment with a larger ovarian cavity.
• When treating, keep warm and oxygen breathing treatment.
• It is surprising to see the effect of the treatment of a newborn baby whose whole body turns blue immediately after undergoing cardiac catheter balloon septal incision surgery treatment and turns to pink skin immediately.
• Hypoglycemia may develop in newborns with large vessel translocations.
• Preventive treatment of hypoglycemia with blood glucose injection.
• After receiving emergency cardiac catheter treatment, the venous blood from the whole body flows to the left atrium and arterial blood from the lungs flows to the right atrium. Treats palliative heart surgery.
• There are many other types of palliative surgery treatments.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제7권 소아청소년 감염병
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert Murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”