급성 충수염 Acute appendicitis
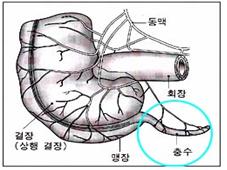
그림 196. ◯으로 표시한 부위에 충수가 있다.
충수를 맹장이라고 부르기도 한다. 그러나 충수와 맹장은 다르다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
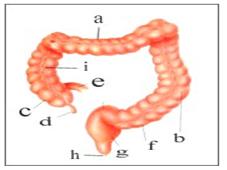
그림 197. 대장관과 충수 구조
a-횡행결장, b-하행결장, c-맹장, d-충수, e-회장, f-S상 결장, g-직장, h-항문, i-상행결장
출처-Used with permission from 소아 가정간호백과와 Galaxo Wellcome
-
충수는 상행 결장의 기시 부위에 달려있는 상행 결장의 일부분이다. 즉 작은 장관이다. 성인 충수의 2~20cm정도, 평균 길이는 8.3cm이다. 충수관 기시부는 상행 결장관에 연결되고 충수관 맨 끝 부위는 막혀 있다.
-
여기에 생긴 염증을 충수염이라고 한다.
-
충수관 속에 박테리아나 드물게는 요충 또는 그 외 다른 종류의 병원체가 감염되면 충수염이 생길 수 있다.
-
충수염이라고 부르는 대신 맹장염이라고 전에는 불렀다.
급성 충수염의 원인
-
어떤 사람들은 충수염에 걸리고 어떤 사람들은 충수염에 걸리지 않는다.
-
이유는 아직도 확실히 모른다.
-
대변 덩어리 등으로 충수관 속이 막힐 때 박테리아 감염이 충수관에 생기면 충수염이 생길 수 있다.
-
드물게 충수관의 혈관에 생긴 이상, 충수관의 림프절 비대, 요충이나 충수관 종양 등으로 충수염이 생길 수 있다.
급성 충수염의 증상 징후
-
충수염은 신생아를 비롯하여 어느 연령층 소아청소년들에게 생길 수 있으나 사춘기 아이들과 젊은이들에게 더 잘 생긴다.
-
충수염의 증상 징후는 다양하다. 영유아의 충수염의 증상 징후는 더 다양하고 복잡하다.
-
학령기 아이들이나 사춘기 아이들에게 생긴 충수염의 전형적인 증상 징후는 다음과 같다.
-
초기에 오목가슴이나 윗배, 또는 배꼽주위가 간헐적으로 조금 아프다.(그림 17참조)
-
그 후 배가 점점 더 심하게 아프다 안 아프다 소위 간헐적 복통이 생길 수 있다.
-
이런 식의 복통이 몇 시간 동안 계속된다.
-
충수염이 점점 더 진행되면서 오른쪽 아랫배(하부 복부)가 주로 아프게 된다.
-
충수가 완전히 곪아서 충수염이 터지기 바로 직전이나 터진 후에는 배가 더 심하게 아플 수 있다.
-
이 때 환아 자신이 복부와 몸통을 갑자기 움직이거나, 기침 하면 복부가 울려서 배가 더 아플 수 있다. 오른쪽 고관절과 넓적다리를 오므렸다 쭉 필 때 오른쪽 아랫배가 당기고 아플 수 있다.
-
이 때 손으로 오른쪽 아래 복부를 누르면 심하게 아프다.
-
미열 내지 고열이 날 수 있다.
-
곪은 충수관을 수술로 떼어 내는 치료를 받을 때까지 계속 열이 난다.
-
입맛이 떨어지고 구역질과 구토할 수 있다.
-
정상으로 대변을 보든지 변비 변, 또는 설사 변을 볼 수 있다.
-
적기에 충수염 수술 치료를 받지 않으면 곪은 충수관이 터지고 복막염, 복강 내 농양 등이나 그 외 다른 여러 가지 합병증이 생길 수 있다.
-
복막염이나 복강 내 농양을 일으킨 박테리아가 전신으로 퍼져 패혈증 등 다른 박테리아 감염병을 일으킬 수 있다.
-
충수염을 일으킨 박테리아가 방광 주위로 퍼져 방광 주위 복막염이 생기면 소변이 자주 마려울 수 있다.
-
신생아들, 영아들, 학령기 이전 유아들이 충수염에 걸리면 앞서 설명한 전형적 증상 징후과 같은 증상 징후가 나타나지 않을 때가 많다.
급성 충수염의 진단
-
병력, 증상 징후, 진찰소견 등을 종합해서 충수염이 의심되면 CBC 피 검사, 소변검사, 복부와 골반강 X-선 사진검사, 복부 초음파 사진, CT 스캔 검사 등으로 진단할 수 있다.
-
일반적으로 충수염이 막 시작할 때나, 그 후 얼마 동안, 또는 특히 영유아들이 충수염에 걸렸을 때는 충수염을 금방 확실히 진단하기가 쉽지 않다.
-
충수염의 초기 증상 징후는 다른 종류의 감염병 특히 복강 내 감염병의 증상 징후와 비슷한 때가 많다.
-
또 영유아들에게 충수염이 생길 때는 앞서 설명한 전형적인 증상 징후가 잘 나타나지 않는 때가 많다.
-
오른쪽 폐에 생긴 폐렴이 있을 때도 충수염의 증상 징후와 거의 비슷하게 오른쪽 상 복부, 아래쪽 하복부가 아플 수 있다.
-
복강 내 림프절이 곪을 때, 류마티스 열이 있을 때도 충수염의 증상 징후와 거의 비슷한 증상 징후가 생길 수 있다.
-
그 외 다른 병들의 증상 징후도 충수염의 증상 징후와 거의 비슷한 때가 많다.
-
충수염에 걸렸다고 의심되면 의사의 진단 치료를 곧 받아야 한다.
-
어떤 때는 충수염을 앓는지 금방 확실히 진단할 수 없기 때문에 병원에 입원해 그 병의 진행 상태를 관찰하면서 재 진찰을 하고, 임상검사, 복부 X-선 사진, 초음파 사진 등을 다시 검사해서 진단할 때도 있다.
급성 충수염의 치료
-
탈수 치료를 하고 예방하기 위해 포도당 전해질용액 정맥주사를 준다.
-
열이 나고 아프면 해열 진통제로 치료한다.
-
4세 이전 영유아들의 충수염은 처음으로 진단을 붙일 때 65% 정도 충수염이 이미 터지고 나이가 어리면 어릴수록 확진 붙이기 전에 이미 터져있는 확률이 더 높다고 한다(Pediatric News, July 2007).
-
충수염이 확진된 후 곪은 충수관은 수술로 제거 치료하는 것이 보통이다.
-
합병증이 없는 충수염은 수술 받은 후 3~4일 정도 될 때 퇴원할 수 있다.
-
터진 충수염은 그때 그 때에 따라 적절히 치료한다.
-
즉 충수염이 터졌을 때 응급 수술치료를 바로 받지 않고 앰피실린(Ampicillin), 클린다마이신(Clindamycin)과 젠타마이신(Gentamicin) 등 3중 광범위 항생제 치료 또는 클린다마이신과 젠타마이신 등 항생제로 치료를 시작해서 염증이 다 가라앉은 다음 8~10주 후에 선별적 충수 절제수술을 받는 방법도 있다.
-
개복수술 충수관 절제 수술치료를 하는 대신 터진 충수염을 복강경 검사법 수술치료법을 이용해서 충수염은 수술하기도 한다.
-
또 충수염이 터져 생긴 복강 내 농양이나 장폐쇄증 등 합병증이 있을 때 적절한 수술 치료를 한다(Pediatric News, July 2007).
-
합병증이 없는 충수염 초기를 항생제로 치료하면 안정성도 있고 치료효과도 좋다는 연구도 있다. Antibiotics Safe and Effective for Uncomplicated Acute Appendicitis. 소스: Physician’s First Watch for April 6, 2012
Acute appendicitis 급성 충수염
Figure 196. There is an appendix in the area marked by ◯. The appendix is sometimes called the appendix. However, the appendix and appendix are different. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 197. Colon and appendix structure a-transverse colon, b- descending colon, c-caecum, d-appendix, e-cause, f-phase colon, g-rectum, h-anus, i-ascending colon Source-Used with permission from Pediatric Home Nursing Encyclopedia and Galaxo Wellcome
• The appendix is the part of the ascending colon that is located at the origin of the ascending colon. That is a small spectacular. Adult appendix is about 2~20cm, and the average length is 8.3cm. The origin of the appendix is connected to the ascending colon and the end of the appendix is blocked.
• This inflammation is called appendicitis.
• Appendicitis can develop when bacteria or, rarely, pinworms or other types of pathogens are infected in the appendix.
• Instead of calling it appendicitis, it was formerly called appendicitis.
Causes of acute appendicitis
• Some people get appendicitis and some don’t.
• I still don’t know why. • Appendicitis can develop if a bacterial infection develops in the appendix when the stool is clogged in the appendix.
• In rare cases, appendicitis may occur due to abnormalities in the blood vessels of the appendix, enlarged lymph nodes in the appendix, or tumors of the pinworm or appendix.
Symptoms signs of acute appendicitis
• Appendicitis can occur in children of any age, including newborns, but is more prevalent in adolescent children and young people.
• Symptoms and signs of appendicitis vary. Symptoms of appendicitis in infants and toddlers are more diverse and complex.
• Typical symptomatic signs of appendicitis in school-age or adolescent children are:
• Initially, the concave chest, upper abdomen, or around the navel is intermittent and a little ache (see Fig. 17).
• After that, the stomach hurts more and more and not sore, so-called intermittent abdominal pain may occur.
• This type of abdominal pain lasts for hours.
• As appendicitis progresses more and more, the right lower abdomen (lower abdomen) usually hurts. • The appendix is completely festered and the stomach may hurt more severely just before or after the appendicitis bursts.
• At this time, if the child suddenly moves his or her abdomen and torso or coughs, the abdomen may ring and the stomach may be more painful. When the right hip joint and thigh are closed and stretched, the right lower abdomen can pull and hurt. • At this time, if you press the lower right abdomen with your hand, it hurts badly.
• You may have a mild or high fever.
• You continue to have a fever until you are treated to surgically remove the festering appendix.
• Loss of appetite and can lead to nausea and vomiting.
• You may have normal stool, constipation, or diarrhea.
• If you do not receive surgical treatment for appendicitis in a timely manner, the festering appendix can rupture, causing peritonitis, abscesses in the abdominal cavity, and other complications.
• The bacteria that caused peritonitis or abscess in the abdominal cavity can spread throughout the body and cause other bacterial infections, such as sepsis.
• If the bacteria that caused appendicitis spread around the bladder, causing peri-bladder peritonitis, urine may often dry out.
• Newborns, infants, and preschool-age infants who develop appendicitis often do not have symptoms, such as the typical symptoms described above.
Diagnosis of acute appendicitis
• If appendicitis is suspected by combining medical history, symptoms, and examination findings, it can be diagnosed with CBC blood test, urine test, abdominal and pelvic cavity X-ray photo test, abdominal ultrasound photo, and CT scan test.
• In general, it is not easy to diagnose appendicitis quickly and reliably when appendicitis is just beginning, for some time thereafter, or especially when infants and toddlers have it.
• Early symptomatic signs of appendicitis are often similar to those of other types of infectious diseases, especially intraperitoneal infections.
• In addition, when infants develop appendicitis, the typical symptomatic signs described above are often less pronounced.
• Pneumonia in the right lung can also cause pain in the upper right and lower abdomen, similar to the symptoms of appendicitis.
• When the lymph nodes in the abdominal cavity are festered, or when you have rheumatic fever, you may have symptoms that are almost identical to those of appendicitis.
• Symptoms of other diseases are often similar to those of appendicitis.
• If you suspect you have appendicitis, you should seek medical attention soon.
• Sometimes it is not possible to quickly diagnose whether you have appendicitis, so you are admitted to the hospital and reexamined while observing the progression of the disease, and even when re-examination of clinical examinations, abdominal x-rays, and ultrasound photographs, etc. have.
Treatment of acute appendicitis
• To treat and prevent dehydration, give an intravenous injection of glucose electrolyte solution.
• If you have a fever and are sick, treat them with antipyretic analgesics.
• Appendicitis in infants and younger children before 4 years of age is said to have already burst at 65% of the time when they are first diagnosed, and the younger they are, the more likely they are to have already burst before the diagnosis (Pediatric News, July 2007).
• After appendicitis is confirmed, the festering appendix is usually removed surgically.
• Uncomplicated appendicitis can be discharged from the hospital 3 to 4 days after surgery.
• Burst appendicitis is treated appropriately, then.
• In other words, when appendicitis breaks out, you do not immediately receive emergency surgical treatment and start treatment with triple broad-spectrum antibiotics such as Ampicillin, Clindamycin, and Gentamicin, or antibiotics such as clindamycin and gentamicin, and the inflammation ends. Another option is to undergo selective appendectomy 8 to 10 weeks after subsidence.
• Instead of performing laparotomy appendectomy surgery, laparoscopic appendectomy is used to treat appendicitis.
• Also, if there are complications such as abdominal abscess or intestinal obstruction caused by a burst of appendicitis, appropriate surgical treatment is performed (Pediatric News, July 2007).
• There are studies showing that treatment of early appendicitis without complications with antibiotics has stability and treatment effect. Antibiotics Safe and Effective for Uncomplicated Acute Appendicitis. Source: Physician’s First Watch for April 6, 2012
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, Harvey grant, and Robert murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 18th edition
-
Red book 29th-31st Ed 2021
- 소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”