급성 중이염 Acute otitis media
급성 중이염의 개요
-
박테리아나 바이러스, 또는 그 외 병원체가 중이 강에 감염되어 생기는 급성 감염병을 급성 중이염이라고 한다.
-
미국에서는 영유들이 항생제 치료를 받아야하는 감염병 중 가장 흔한 감염병이 바로 급성 중이염이다. 급성 중이염의 5~25%는 2차 항생제 치료를 요한다.
-
급성 중이염은 여유아들에게 아주 잘 생길 수 있는 소아 감염병이다.
-
소아청소년과에서 매일 볼 수 있는 소아 감염병이다(출처; Pediatrics. April 2008. p.674).
-
급성 중이염을 일으키는 병원체들 중 가장 흔한 병원체가 박테리아이다.
-
중이강 속으로 박테리아가 침입해서 중이강 속에 감염병이 생기고 중이 속에 고름이 잡힐 수 있다.
-
이 때 생긴 급성 중이염을 항생제로 적절히 치료하지 않으면 고막 감염병이 생길 수 있고, 그래서 박테리아 고막염이 생기고, 그 고막이 파열될 수 있고,
-
급성 중이염이 만성 중이염으로 이어질 수 있고,
-
또 귀가 가늘게 먹든지 심하게 귀 먹을 수 있다.
-
더러 심한 난청 및 농아가 될 수 있다.
-
참고로 여기서 말하는 급성 중이염은 주로 박테리아 중이염을 말한다.
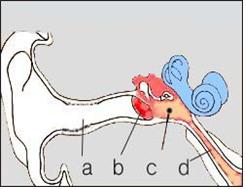
그림 46. 중이염.
a-외이도, b-고막, c-고름이 잡힌 중이염, d-이관(구씨관, Auditory tube).
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
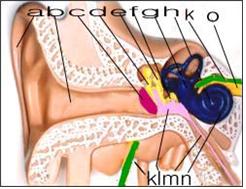
그림 47. 분홍색으로 표시된 부분이 중이염으로 인한 고름.
a-외이, b-외이도, c-고막, d-추골, e-침골, f-등골, g-전정, h-반규관, k-안면신경, l-중이에 괸 고름, m-이관, n-와우, o-청각 신경(제 8 뇌신경).
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 48. 이경.
중이나 외이도, 또는 비강 등을 진찰할 때 주로 쓰는 의료기구.
중이염이나 외이도염 등을 진단하는데 이경을 쓸 수 있고, 외이도 속에 귀지가 조금만 있어도 외이도염이나 중이염을 확실히 진단하는데 지장이 있을 수 있다. 요즘, CompacVideo 이경으로 고막, 외이도 등을 진찰할 수 있고 환자 자신이 직접 비디오를 통해 거기에 이상 여부를 알아볼 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP

사진 49. 이경.
이경에 달려 있는 공기 벌브를 살짝 눌러 공기를 외이도 속에 조금 불어넣으면서 고막이 정상적으로 움직이는지 비정상적으로 움직이는지 않는지 이경 검사를 통해 알아 볼 수 있다. 요즘, CompacVideo 이경으로 고막, 외이도 등을 진찰할 수 있고 환자 자신이 직접 비디오를 통해 거기에 이상이 있는지 없는지 알아볼 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
급성 중이염의 원인
-
연구에 의하면,
-
폐렴연쇄상구균(29.8%),
-
부란햄엘라카탈라리스균(모락셀라카탈라리스균)(11.7%),
-
헤모필러스 인플루엔자균(20.9%),
-
A군 베타 용혈성 연쇄상구균(3.1%),
-
황색 포도상구균(1.6%),
-
또는 슈도모나스에르지노자균(1.2%),
-
대장균 등 중 한 가지 박테리아(세균)가 소아 중이염을 주로 일으킨다.
-
그 중 한 종류의 세균이 한쪽 중이 강이나 양쪽 중이 강에 감염될 때 한쪽 중이나 또는 양쪽 중이에 급성 중이염이 생길 수 있다.
-
폐렴연쇄상구균성 감염을 예방할 수 있는 백신으로 폐렴연쇄상구균 감염으로 생기는 급성 중이염의 발생률은 점점 감소되고 있다.
-
요즘 헤모필러스인플루엔자균 감염으로 생긴 급성 중이염 발생률이 거의 50%이다.
-
바이러스 감염이나 마이코플라스마균 감염으로 급성 중이염이 생길 수 있다.
-
그러나 임상적으로 큰 문제가 되지 않는다.
-
모든 연령층 아이들에게 중이염이 생길 수 있지만 다음과 같은 경우, 급성 중이염이 아이들에게는 더 잘 생긴다.
급성 중이염에 더 잘 걸리게 하는 요건
-
나이가 어릴수록 박테리아 감염에 대한 저항력이 더 약하다. 그래서 영유아들은 급성 중이염에 더 잘 걸릴 수 있다.
-
[부모도 반의사가 되어야 한다–소아가정간호백과]-제6권 신생아 성장 발육 양호 및 질환–신생아 중이염 참조.
-
비정상적으로 커진 아데노이드로 비대, 아데노이드염 또는 인두염 등으로 이관의 입구가 막힐 수 있다. 또 알레르기 비염으로 이관의 입구와 이관이 막히면 중이염이 더 잘 생길 수 있다.
-
이런 이유로 비정상적으로 비대한 아데노이드가 있는 아이들이나 알레르기 비염이 있는 아이들에게 중이염이 더 잘 생긴다.
-
영유아들의 이관의 길이는 영유아기 이후의 학령기 아이들이나 사춘기 아이들, 성인들의 이관의 길이보다 더 짧다.
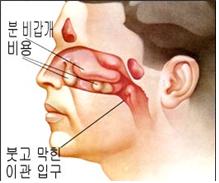
그림 50. 부어 막힌 이관 입구.
Used with permission from Schering Corporation, NJ. USA
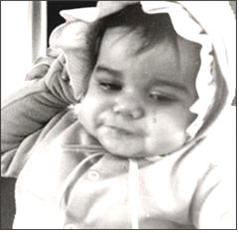
사진 51. 급성 중이염을 앓을 때 귀가 아파서 울기도 하고, 귀를 잡아당길 수 있다. 그러나 귀를 잡아당기는 징후는 중이염의 징후 뿐 아니라 다른 이유로도 귀를 잡아당긴다.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
-
영유아들의 인두나 비강에 감염됐던 박테리아가 짧은 이관을 쉽게 통과해서 중이 속으로 쉽게 침입할 수 있다.
-
영유아들은 각종 세균 감염에 저항할 수 있는 면역체를 충분히 가지고 있지 않다. 그래서 영유아들은 중이염에 더 잘 걸린다.
-
영유아들의 이관은 성인들의 이관보다 더 가늘기 때문에 감기나 다른 종류의 바이러스 상기도염, 부비동염(축농증), 알레르기 비염 등으로 이관이 쉽게 붓고 막히게 된다. 이 때 중이강 속의 압이 음압으로 되고 중이강 내 삼출액이 생길 수 있다. 박테리아가 이관을 통과해서 중이강 속으로 쉽게 침입할 수 있고 중이강 속에 괸 삼출액은 박테리아가 자라는데 좋은 배양지가 된다. 이런 이유로 중이염이 더 쉽게 생길 수 있다.
-
엄마의 젖을 먹고 대신 우유 단백질 인공영양을 먹는 영아들, 아토피성 체질을 가진 영유아들, 기관지 천식, 알레르기 비염, 아토피성 피부염 등의 알레르기 질환을 가지고 있는 영유아들이 감기 등 바이러스 상기도 염 등을 앓을 때 중이염에 더 잘 걸릴 수 있다.
-
친 부모 형제자매들 중 누구든 중이염을 자주 앓았던 가족 병력이 있으면 다른 친 형제 자매들은 중이염에 더 잘 걸린다.
-
영유아들이 노리개 젖꼭지를 빨면 중이염에 더 잘 걸릴 수 있다. 그러나 어떤 연구에는 중이염에 덜 걸린다고 한다.
-
그 외 다른 이유로 영유아들이 중이염에 잘 걸릴 수 있다.
급성 중이염의 증상 징후
-
소아들에게 생기는 급성 중이염의 증상은 나이 등에 따라 다양하다.
-
급성 중이염만 앓을 수 있지만 중이염은 알레르기 비염이나 기관지 천식, 또는 아토피성 피부염 등 알레르기 질환이 있는 아이들에게 더 잘 생긴다.
-
감기나 다른 종류의 바이러스 상·하기도 염 등을 앓을 때 그런 병의 이차 박테리아 감염 등으로 생긴 합병증으로 중이염이 생길 수 있다.
-
그 밖에 구개 열 등 다른 동반 질환이 있을 때 중이염을 동시 앓을 수 있다.
-
중이염을 앓을 때 중이염과 같이 있는 병의 증상 징후가 중이염의 증상과 함께 나타날 수 있다.
-
어떤 아이들의 급성 중이염의 증상 징후는 전형적으로 나타나지 않는다. 그래서 신생아들이나 영아들이 급성 중이염을 앓을 때 외이도 속, 고막, 중이를 자세히 진찰하지 않고 중이염을 앓고 있는지 모르고 지나 갈 수 있다. 이런 이유로 감기를 앓는 영유아들이 소아청소년과에서 진료받을 때는 감기뿐만 아니라 중이염이 있나 환인하기 위해 이경으로 외이도와 고막을 꼭 진찰한다.
-
소아 건강검진을 정기적으로 받기 위해 소아청소년과에 영유아를 데리고 왔다가 중이염이 있는 것을 처음 진단 받을 때도 있다.
-
진단 받지 않고 치료 받지 않은 중이염으로 청력이 심하게 감소된 아이들은 TV를 크게 틀어놓고, 수업 시간에 교사들의 말을 전혀 알아듣지 못할 수 있고, 대화 할 때 말하는 사람의 입술과 행동을 보고 대화 상대자가 무슨 말을 하고 있는지를 눈치로 알아듣기도 한다.
-
어려서 아직 말로 자기 의사를 잘 표현할 줄 모르는 영유아들이 감기나 독감, 또는 다른 종류의 바이러스 상·하기도 염을 앓는 중 박테리아가 중이강 속에 침입해서 급성 중이염에 걸릴 수 있다.
-
영아들이 갑자기 급성 중이염에 걸리면 귀가 몹시 아파서 몹시 보채고 울고, 짜증내고, 귀를 비비고, 자다가 자주 깰 수 있다.
-
말로 자기 의사를 표현할 줄 아는 유아들이 급성 중이염에 걸리면 귀가 아프다고 호소한다. 또 귀에서 이상한 소리가 나고, 잘 들리지 않는다고 말할 수 있다.
-
급성 중이염이 있을 때 미열, 두통, 구토, 복통 등의 증상 징후가 함께 나타날 수 있다.
-
그렇지만 급성 중이염 그 자체로 고열이 나는 때는 드물다.
-
급성 중이염이 있을 때 급성 중이염과 같이 있는 바이러스 상·하기도 염으로 열이 나는 경우가 더 많다.
-
특히 박테리아 급성 중이염을 조기에 속히 진단해서 적절히 치료하지 않으면 고막이 터질 수 있다. 박테리아 급성 중이염으로 고막이 터지면 피 섞인 고름이 중이강 속에서 외이도 속으로 흘러나오고 그 고름이 귓구멍 밖으로 흘러나올 수 있다.
-
이것을 귀젖, 귓물 또는 이루라고 한다.
-
열이 나면서 박테리아 급성 중이염이 앓을 때 고막이 터져 중이강 속에 있는 고름이 외이도 속으로 흘러나올 때 그 동안 났던 열이 떨어지고 중이강 속에 있는 고름이 외이도 속으로 흘러나오면 그 동안 났던 열이 내리고 귀가 덜 아플 수 있다.
-
박테리아 급성 중이염을 적절히 치료해 주지 않고 오랫동안 방치하면 급성 중이염이 만성 중이염으로 변할 수 있고 난청, 유양돌기염, 뇌막염 등 합병증이 생길 수 있다.
-
급성 중이염이 만성 중이염으로 되면 고막이 만성으로 뚫려 있을 수 있다.
-
이 때 만성 중이염으로 뚫린 고막 구멍을 통해서 중이강 속에서 고름이 외이도 속을 통해서 귓구멍 밖으로 오랫동안 흘러나올 수 있다.
급성 중이염의 진단
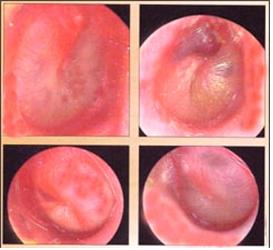
사진 52. 급성 중이염으로 고막이 빨갛게 붓고 부푼다.
출처– Otitis Media, Roche laboratories
-
병력, 보챔, 귀가 아프고 청력 감소 등의 증상 징후와 다음과 같은 진찰소견 등을 종합하여 급성 중이염을 쉽게 진단할 수 있다.
-
이경으로 외이도 속을 통해 고막을 육안으로 들여다보고 고막을 통해 중이강 속에 든 고름을 보고 진단한다.
-
소아청소년과에서 외이도 내 귀지가 가득히 차 있거나 중이 강을 적절히 진찰할 수 없을 때는 증상 징후로 참작해서 추정진단 할 수 있고 귀지를 귀 큐렛(curette) 등으로 제거하거나 그 외 다른 방법으로 귀지를 제거하고 고막을 드려다 보고 진단할 때도 있다.
-
급성 중이염이 있을 때 고막을 이경으로 들여다보면서 진찰을 해보면 중이염이 있는 귀 쪽 고막이 외이도 속 쪽으로 불룩 팽배되어 있고 고막이 빨갛게 붓고 중이강 속에 고름이 잡혀 있는 것을 눈으로 직접 볼 수 있다 사진 52 참조 .
-
이경에 달린 공기 밸브로 공기를 외이도 속으로 살짝 불어 고막의 움직임을 보면 중이 속에 고름이나 삼출액이 들어있는지 검사할 수 있다.
-
즉, 고막이 잘 움직이지 않거나 거의 움직이지 않고 중이 내에 공기와 삼출액, 또는 고름이 차있는 것을 볼 수 있고 때로는 고막이 터져 터진 고막 구멍을 통해 중이강 속 고름이 외이도 속으로 흘러나오는 것도 볼 수 있다(그림 72 참조).
|
귀 내시경 영상에서 본 고막에서도 이경으로 본 고막에서도 고막 팽창이 중이염 진단에 가장 가치가 있다고 한다. |
급성 중이염의 치료
-
중이염이 급성인가 만성인가, 경미한지 심한지, 중이염을 앓는 자녀의 나이, 중이염을 일으킨 병원균, 또 중이염이 있으면서 합병증의 유무에 따라 치료를 다르게 할 수 있다.
-
급성 중이염으로 그 쪽 귀가 아프고 열이 날 때는 타이레놀이나 모트린 등 진통제로 진통과 해열을 우선 시킬 수 있다.
-
국소 마취제 Topical lidocain 2% 귀 점적액제로 중이염으로 생긴 통증을 응급 치료 할 수 있다.
-
경구용 진통제와 국소 마취제 Lidocain으로 이통을 치료 할 수 있다(출처; Infectious disease in children, July 2008).
-
급성 중이염이 경미하고 페니실린 알레르기가 없으면 경구용 아목시실린(Amoxicillin) 등 항생제로 치료할 수 있다.

그림 53. 의사 처방한 항생제를 섬취하라는 기간 동안 섭취 해야 한다.
Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
-
중이염이 심하지 앓고 페니실린 알레르기가 없으면 최초 선택용 항생제는 Augmentin(amoxicillin/clavulanate)이다.
-
페니실린에 알레르기가 있으면 Ceftriaxone 주사, Cefdinir, Cefuroxime axetil, Cefpodoxime proxetil, Clindamycin, Azithromycin, Clarithromycin, 또는 Gatifloxacin 등 중 한 가지의 항생제를 최초 선택용 항생제로 치료할 수 있다.
-
그 외 Septra나 Erythromycin-sulfisoxazole 등 항생제를 최초 선택용으로 치료 한다.
-
급성 중이염을 일으킨 박테리아를 죽일 수 있는 항생제 치료를 시작한지 2~3일이 지나면 증상 징후가 거의 없어지는 것이 보통이다.
-
그렇지만 급성 중이염이 완전히 다 완치되기까지는 의사가 처방한 항생제로 완전히 치료해야 한다.
-
항생제로 치료한 후 중이염이 완치되었는지 확인하기 위해 의사의 따라잡기 진단치료를 꼭 받아야 한다.
- 폐렴연쇄상구균, 부란햄엘라카탈라리스균, 또는 헤모필러스인플루엔자균 등의 감염으로 생긴 중이염은 경구용 아지스로마이신(Azithromycin) 등으로 치료할 수 있다.
|
급성 중이염을 치료할 때 아지스로마이신의 용량
|
-
이상 설명한 바와 같이 급성 중이염 치료에 쓸 수 있는 최초 선택용 항생제의 종류는 환아가 사는 나라, 지방, 시기 등에 따라 또는 다른 조건에 따라 자주 바꿔질 수 있다.
-
그래서 급성 중이염 치료에 쓰는 항생제의 최초 선택 항생제의 종류는 전적으로 의사에게 맡겨야 한다.
-
어떤 의사는 적절한 항생제로 적절히 치료를 한 후 증상 징후가 없으면 의사의 따라잡기 재 진찰을 꼭 받을 필요가 없다고 주장한다.
-
그러나 항생제로 치료를 받은 후 아무 증상 징후가 없더라고 완치됐는지 알아보기 위해 의사의 따라잡기 진찰을 꼭 받아야 한다.
-
어떤 아이들은 급성 중이염이 시작될 때 얼마 동안 귀가 아프다고 호소하다가 그 이후부터는 더 이상 귀가 아프다고 호서 하지 않고 보통 때와 같이 지내는 경우도 있다.
-
그러다가 그 후 얼마 있다가 “남들이 하는 말을 잘 알아듣지 못하거나 텔레비전을 크게 틀어놓는다.”고 부모가 아이를 소아청소년과에 데리고 왔을 때 급성 중이염이 있다는 것을 처음 진단받고 치료를 시작하는 경우도 있다.
-
항히스타민제나 비강 점막 출혈완화제는 급성중이염 치료에 별 효과가 없다고 한다.10과 30.
-
급성 중이염이 만성 중이염으로 진행되면 고막이 뚫리고 뚫린 고막 구멍을 통해 중이강 속 고름이 외이도 속으로 흘러나오거나 유양돌기염, 골수염, 뇌막염 등의 합병증이 생길 수 있다.
그림 54. 중이염으로 청력이 감소될 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
-
이런 합병증이 생길 때는 병원에 입원해서 수술 및, 또는 항생제로 치료받아야 한다.
-
급성 중이염으로 뚫린 고막은 급성 중이염을 적절히 치료한 후 저절로 막히는 것이 보통이다.
-
급성 중이염으로 생기는 심한 귀 통증을 CO2 레이저 치료를 받으면 1시간 내에 그 통증이 가신다고 한다.
-
레이저로 고막 절개수술 치료, 통기관 삽입수술로 치료할 수 있고 중이강 내 고름을 빼낼 수 있다.
-
폐렴연쇄상구균 백신으로 예방접종을 기본으로 받아서 삼출성 급성 중이염의 재발은 방지할 수 없다는 연구결과도 있다.
|
다음은“중이염”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 중이염
Q.
- 17개월 된 아기입니다.
- 감기에 걸리면 꼭 중이염이 되곤 합니다. 올해 들어 3번 감기에 걸렸는데 3번 다 중이염으로 되었습니다.
- 의사선생님께서 새로 나온 폐구균 백신이 있다고 접종해 주면 어느 정도 예방은 된다던데 어떻게 하는 것이 좋을까요?
- 답변 부탁드립니다…
A.
- 명희님
- 안녕하세요. 질문해 주셔 감사합니다.
- 자녀의 나이, 성별, 과거와 가족의 병력, 진찰소견, 임상검사 결과 등 많은 정보가 있으면 더 좋은 답변을 드릴 수 있습니다. 주신 정보를 참작해 답변을 드립니다.
■ 중이염을 일으키는 세균
- 폐렴연쇄상구균(29.8%)이 가장 흔한 박테리아 원인균입니다.
- 폐렴연쇄상구균 감염에 의해서 생기는 급성 중이염은 폐렴연쇄상구균 백신으로 예방접종을 받으면 어느 정도 폐렴연쇄상구균성 중이염의 예방이 될 수 있습니다.
- 그러나 폐렴연쇄상구균의 균종이 많이 있고 그 폐렴 백신 예방접종으로 모든 균종의 감염으로 생긴 폐렴 연쇄상구균성 중이염이 다 예방될 수 없습니다.
- 폐렴 연쇄상구균 백신으로 예방접종을 받기 시작한 이후부터 급성 중이염의 발생률이 다소 감소됐다는 연구는 있습니다.
- 다시 말씀드리면 폐렴 연쇄상구균 백신 예방접종으로 중이염의 발생률을 다소 감소시킬 수는 있지만 폐렴 연쇄상구균 백신 예방접종으로 모든 균 종류의 폐렴 연쇄상구균성 중이염을 다 예방할 수 없고 폐렴 연쇄상구균 감염 이외 다른 세균 감염에 의해서 급성 중이염이 생길 수 있습니다.
- 폐렴 연쇄상구균성 중이염을 예방해주기 위해서 폐렴 예방접종백신으로 예방접종을 잘 받아야 할뿐만 아니라 폐렴 연쇄상구균성 뇌막염이나, 폐렴 등을 예방해주기 위해서 폐렴 연쇄상구균백신 예방접종을 받는 것을 권장합니다.
- 중이염은 다음과 같이 여러 종류의 세균들 중 한두 종류에 의해서 생길 수 있습니다.
- 폐렴연쇄상구균(29.8%),
- 부란햄엘라카탈라리스균(모락셀라카탈라리스균)(11.7%),
- 헤모필러스 인플루엔자균(20.9%),
- A군 베타 용혈성 연쇄상구균(3.1%),
- 황색 포도상구균(1.6%),
- 슈도모나스에르지노자균(1.2%),
- 대장균 등 세균이 소아 중이염을 주로 일으킵니다.
- 그 중 한 종류의 세균이 한쪽 중이나 양쪽 중이에 감염될 때 중이염이 생길 수 있습니다.
- 괄호 내 %는 중이염을 일으키는 박테리아의 퍼센트입니다(출처-Bluestone CD, Klein JO).
- 소아들에게서 중이염이 잘 생기는 이유와 원인에 관해서 p.00 급성 중이염의 정보를 참조하시기 바랍니다.
- 바이러스나 마이(미)코플라스마균으로도 급성 중이염이 생길 수 있고 모든 연령층의 아이들에게 중이염이 생길 수 있지만 다음과 같은 아이들은 급성 중이염에 더 잘 걸립니다.
■ 급성 중이염에 더 잘 걸릴 수 있는 조건.
- 나이가 어릴수록 박테리아의 침입에 대한 저항력이 더 약하고 특히 영유아들에게 급성 중이염이 더 잘 생길 수 있습니다(p.00 신생아 중이염 참조).
- 비정상적으로 커진 아데노이드로 이관 입구가 더 쉽게 막힐 수 있습니다. 그 외 알레르기 비염 등 다른 원인으로 이관이 막혀 중이염이 더 잘 생길 수 있습니다. 이런 이유로 비정상적으로 비대한 아데노이드가 있는 아이들에게 중이염이 더 잘 생깁니다.
- 영유아들의 이관의 길이는 영유아기 이후 학령기나 사춘기 아이들이나 성인들의 이관의 길이보다 더 짧습니다. 영유아들의 인두나 비강에 있는 박테리아가 짧은 이관을 쉽게 통과해서 중이강 속으로 쉽게 침입할 수 있습니다.
- 그래서 영유아들은 중이염에 더 잘 걸립니다.
- 또 영유아들의 이관은 성인들의 이관보다 더 가느다랗습니다.
- 감기나 다른 종류의 바이러스성 상기도 염, 부비동 염(축농증), 알레르기 비염 등을 앓을 때 이관이 쉽게 붓고 막힐 수 있습니다.
- 이 때 중이강 속의 압이 음압으로 변하고 중이강 속에 삼출액이 고이게 되고 그 삼출액은 이관을 통과해서 중이강 속으로 들어온 박테리아가 자라는데 좋은 배양지가 됩니다. 이런 이유로 중이염이 더 쉽게 생길 수 있습니다.
- 엄마 젖을 먹는 대신 우유 단백질이 든 인공영양을 먹는 영아들, 아토피 체질을 가진 영유아들, 기관지 천식, 알레르기 비염, 아토피성 피부염 등의 알레르기 질환을 가지고 있는 영유아들이 감기 등 바이러스성 상기도 염 등을 앓을 때 중이염에 더 잘 걸릴 수 있습니다.
- 친 부모 형제자매들 중 누군가가 중이염을 자주 앓은 병력이 있으면 다른 형제자매들도 중이염에 더 잘 걸립니다.
- 영유아들이 노리개 젖꼭지를 빨면 중이염에 더 잘 걸릴 수 있다고도 하고 덜 걸릴 수 있다는 상반된 연구도 있습니다. 영유아들에게 그 외 다른 원인으로 중이염이 더 잘 걸릴 수 있습니다.
- 급성 중이염 참조.
- 더 자세한 것은 소아청소년과 에서 상담하시기 바랍니다.
- 질문이 더 있으면 또 방문하세요. 감사합니다. 이상원 드림
Acute otitis media 급성 중이염
Overview of Acute Otitis Media
• Acute otitis media caused by bacteria, viruses, or other pathogens infecting the middle ear cavity is called acute otitis media.
• In the United States, acute otitis media is the most common infectious disease among infants requiring antibiotic treatment. 5-25% of acute otitis media require second-line antibiotic therapy.
• Acute otitis media is a pediatric infectious disease that can occur very frequently in young children.
• It is a pediatric infectious disease that can be seen every day in the Department of Pediatrics (source; Pediatrics. April 2008. p.674).
• Bacteria are the most common pathogens that cause acute otitis media.
• Bacteria can enter the middle ear cavity, causing infectious disease in the middle ear cavity and collecting pus in the middle ear.
• If acute otitis media at this time is not properly treated with antibiotics, an infection of the eardrum may occur, which may result in the bacterial eardrum, the eardrum may rupture,
• Acute otitis media can lead to chronic otitis media;
• You may also have thin or severely deaf ears.
• More severe hearing loss and deafness.
• For reference, acute otitis media referred to here mainly refers to bacterial otitis media.
Figure 46. Otitis media. a-external auditory canal, b-tympanic membrane, c-pus-filled middle ear cavity, d-ear canal (Auditory tube). Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Figure 47. The area marked in pink is pus due to otitis media. a-external ear, b-external auditory meatus, c-tympanic membrane, d-vertebral column, e-incus, f-stapes, g-vesicle, h-semicircular duct, k-facial nerve, l-middle ear pus, m-Eustachian duct, n- cochlear, o-auditory nerve (8th cranial nerve). Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 48. Lee Kyung. A medical instrument mainly used to examine the middle, external auditory canal, or nasal cavity. An otoscope can be used to diagnose otitis media or otitis externa, and even a small amount of earwax in the external auditory meatus can interfere with a definitive diagnosis of otitis externa or otitis externa. Nowadays, the CompacVideo otoscope can examine the tympanic membrane and the ear canal, and the patient himself can see if there are any abnormalities through the video. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Photo 49. Lee Kyung. You can check whether the eardrum is moving normally or abnormally through an otoscope by gently pressing the air bulb on the ear canal and blowing a little air into the ear canal. Nowadays, the CompacVideo otoscope can examine the tympanic membrane, the ear canal, and the like, and the patient himself can see if there is anything wrong with the video. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Causes of acute otitis media
• According to research,
• Streptococcus pneumoniae (29.8%);
• Buranham ella catalaris (Moraxella catallaris) (11.7%),
• Haemophilus influenzae (20.9%),
• group A beta-hemolytic streptococci (3.1%);
• Staphylococcus aureus (1.6%);
• or Pseudomonas erginosa (1.2%);
• One type of bacteria (bacteria), such as E. coli, mainly causes otitis media in children.
• Acute otitis media can occur in one or both middle ears when one type of bacteria infects one or both middle ear cavities.
• As a vaccine that can prevent pneumococcal infection, the incidence of acute otitis media caused by streptococcal infection is gradually decreasing.
• Nowadays, the incidence of acute otitis media caused by Haemophilus influenzae infection is nearly 50%.
• Acute otitis media can be caused by viral infection or mycoplasma infection.
• However, it is not a major clinical problem.
• Children of all ages can develop otitis media, but children are more likely to develop acute otitis media if: Requirements that predispose you to acute otitis media
• The younger you are, the less resistant you are to bacterial infections. Therefore, infants and young children are more susceptible to acute otitis media. • www.drleepediatrics.com – Volume 6 Newborn growth and development and diseases – See otitis media in newborns.
• Abnormally enlarged adenoids, such as hypertrophy, adenoiditis, or pharyngitis, may block the entrance to the ear canal. In addition, if the entrance of the ear canal and the ear canal are blocked by allergic rhinitis, otitis media may be more likely to occur.
• For this reason, children with abnormally enlarged adenoids or children with allergic rhinitis are more likely to develop otitis media.
• The length of transfer for infants and toddlers is shorter than that for school-age children after infancy, puberty, and adults.
Figure 50. Swollen clogged eustachian tube entrance. Used with permission from Schering Corporation, NJ. USA
Picture 51. When you have acute otitis media, you may cry because your ears hurt, and you may pull your ears. However, signs of pulling ears are not only signs of otitis media, but also pulling ears for other reasons. Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
• Bacteria that have been infected in the pharynx or nasal passages of infants and young children can easily pass through the short ear canal and easily enter the middle ear. • Infants and young children do not have enough immune systems to resist various bacterial infections.
Therefore, infants and young children are more susceptible to otitis media. Because the ear canal of infants and young children is thinner than that of adults, the ear canal is easily swollen and blocked due to colds or other viral upper respiratory tract infections, sinusitis (sinusitis), and allergic rhinitis. At this time, the pressure in the middle ear cavity becomes negative pressure, and effusion may occur in the middle ear cavity. Bacteria can easily enter the middle ear cavity through the ear canal, and the exudate in the middle ear cavity is a good culture medium for bacteria to grow. For this reason, otitis media may be more likely to develop.
• Infants who drink their mother’s milk and take milk protein supplements instead, infants with atopic constitution, and infants with allergic diseases such as bronchial asthma, allergic rhinitis, and atopic dermatitis may suffer from viral upper respiratory tract infections such as colds. You may be more prone to otitis media.
• If any of your biological parents’ siblings have a family history of frequent otitis media, the other biological siblings are more likely to get otitis media.
• Infants and toddlers may be more susceptible to otitis media if they suck on a soother. However, some studies suggest that they are less prone to otitis media.
• For other reasons, young children are more prone to otitis media. Symptoms of acute otitis media
• Symptoms of acute otitis media in children vary according to age. • You can only get acute otitis media, but otitis media is more common in children with allergies, such as allergic rhinitis, bronchial asthma, or atopic dermatitis. • When you have a cold or other viral upper and lower respiratory tract infections, you may develop otitis media as a complication caused by secondary bacterial infection of those diseases.
• You may have otitis media at the same time when you have other comorbidities such as cleft palate.
• When you have otitis media, symptoms of a disease that coexists with otitis media may appear along with the symptoms of otitis media.
• Symptoms of acute otitis media in some children are not typically present. Therefore, when newborns or infants suffer from acute otitis media, they may pass without knowing whether they have otitis media without thoroughly examining the inner ear canal, tympanic membrane, and middle ear. For this reason, when infants and young children with colds are treated at the Department of Pediatrics, they must examine the ear canal and eardrum with an otoscope to check for otitis media as well as colds.
• Otitis media is sometimes diagnosed for the first time after bringing an infant to the Department of Pediatrics for regular pediatric health check-ups. • Children with severe hearing loss due to undiagnosed and untreated otitis media may have the TV turned on loudly, they may not be able to understand teachers at all in class, and the lips and behavior of the person speaking to the conversation may not help the person they talk to. You can even hear what you are saying with your eyes.
• Infants and young children who are still young and do not know how to express themselves well in words can get acute otitis media when bacteria enter the middle ear cavity while they are suffering from a cold, flu, or other viral upper and lower respiratory tract infections.
• If infants suddenly develop acute otitis media, their ears may be very sore, and they may sneeze, cry, become irritable, rub their ears, and often wake up from sleep.
• Infants who can express themselves verbally complain of ear pain when they get acute otitis media. You may also hear strange noises in your ears and say you can’t hear well.
• When acute otitis media is present, symptoms such as low fever, headache, vomiting, and abdominal pain may appear together.
• However, acute otitis media itself rarely causes high fever.
• When acute otitis media is present, fever is more common due to viral upper and lower respiratory tract infections with acute otitis media.
• Especially if acute bacterial otitis media is not diagnosed and treated promptly, the eardrum can burst. When the eardrum ruptures due to bacterial acute otitis media, bloody pus flows from the middle ear cavity into the external auditory meatus, and the pus can flow out of the ear canal.
• This is called the udder, eardrum, or ear canal. • When you have a bacterial acute otitis media with fever when the eardrum ruptures and pus in the middle ear cavity flow into the ear canal, the fever that has been in the past drops and the pus in the middle ear cavity flows into the ear canal .
• If bacterial acute otitis media is left untreated for a long time without proper treatment, acute otitis media may turn into chronic otitis media, and complications such as hearing loss, mastitis, and meningitis may occur.
• If acute otitis media becomes chronic otitis media, the eardrum may be chronically punctured.
• In this case, pus can flow out of the ear canal through the ear canal through the eardrum hole due to chronic otitis media for a long time.
Diagnosis of acute otitis media
Photo 52. Red, swollen and swollen eardrum with acute otitis media. Source- Otitis Media, Roche laboratories • Acute otitis media can be easily diagnosed by synthesizing the medical history, symptoms, and symptoms such as hearing loss and hearing loss as well as the following examination findings.
• Diagnosis is made by visually examining the eardrum through the inner ear canal with an otoscope and looking at the pus in the middle ear cavity through the eardrum.
• When the earwax in the external auditory meatus is full or the middle ear cavity cannot be properly examined in the Department of Pediatrics, a presumptive diagnosis can be made by considering the symptoms and removing the earwax with an ear curette or other methods. There are times when a diagnosis is made by looking at the eardrum.
• In case of acute otitis media, if you examine the tympanic membrane with an otoscope, you can directly see that the tympanic membrane on the side of the ear with otitis media bulges into the inside of the external auditory meatus, the tympanic membrane swells red and pus is trapped in the middle ear cavity. See Photo 52 .
• You can check the middle ear for pus or exudate by gently blowing air into the ear canal with an air valve attached to the ear canal and observing the movement of the eardrum.
• In other words, the eardrum does not move well or hardly moves, and the middle ear can be seen filled with air, exudate, or pus, and sometimes pus from the middle ear cavity can be seen through the ruptured eardrum opening into the ear canal (Fig. 72). It is said that the tympanic membrane is the most valuable for diagnosing otitis media, both in the tympanic membrane as seen in the endoscopic image, and in the tympanic membrane seen through the otoscope. sauce; Infectious Diseases In Children, Vol.24.#9. September 2011 Treatment of acute otitis media
• Treatment may vary depending on whether otitis media is acute or chronic, mild or severe, the age of the child with otitis media, the pathogen that caused otitis media, and the presence or absence of complications with otitis media. • If you have a sore ear and fever due to acute otitis media, you can prioritize pain relief and fever relief with painkillers such as Tylenol or Motrin.
• Local anesthetic Topical lidocain 2% ear drops can provide emergency treatment for pain caused by otitis media.
• Ear pain can be treated with oral analgesic and local anesthetic Lidocain (source; Infectious disease in children, July 2008).
• If acute otitis media is mild and there is no penicillin allergy, it can be treated with antibiotics such as oral amoxicillin.
Figure 53. Antibiotics prescribed by a doctor should be taken for the duration of the prescribed period. Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
• If you have mild otitis media and do not have penicillin allergy, the first antibiotic of choice is Augmentin (amoxicillin/clavulanate).
• If you are allergic to penicillin, Ceftriaxone injection, Cefdinir, Cefuroxime axetil, Cefpodoxime proxetil, Clindamycin, Azithromycin, Clarithromycin, or Gatifloxacin may be treated as first-line antibiotics.
• In addition, antibiotics such as Septra or Erythromycin-sulfisoxazole are used as the first choice.
• Symptoms usually disappear within 2-3 days of starting antibiotic therapy, which can kill the bacteria that caused acute otitis media.
• However, until acute otitis media is completely cured, it must be completely treated with antibiotics prescribed by a doctor.
• After treatment with antibiotics, it is essential to receive a follow-up diagnostic treatment from a doctor to confirm that the otitis media has been cured.
• Otitis media caused by infections such as Streptococcus pneumoniae, Buranham ella catalaris, or Haemophilus influenzae can be treated with oral azithromycin.
Dosage of azithromycin to treat acute otitis media
① Take 30mg per kg of body weight once or
② Take 10 mg per kg of body weight as a daily supply for the next 3 days or
③ Take 10 mg/kg of body weight on the first day and 5 mg/kg of body weight on the 2nd, 3rd, 4th, and 5th days. Also, there is a study that shows good treatment results for acute otitis media with a single dose of oral azithromycin.
• As described above, the types of antibiotics for the initial selection that can be used for the treatment of acute otitis media can be changed frequently depending on the country, region, period, etc. where the child lives or other conditions.
• Therefore, the type of antibiotic of first choice for the treatment of acute otitis media should be left entirely to the doctor.
• Some doctors assert that, after adequate treatment with appropriate antibiotics, there is no need to see a doctor for follow-up re-examination if there are no signs of symptoms.
• However, after you have been treated with antibiotics, even if you have no symptoms, you should definitely see a follow-up with your doctor to see if you are cured.
• At the onset of acute otitis media, some children complain of ear pain for a while, and after that, they no longer complain of ear pain and go on as usual.
• Then, after a while, when parents bring their child to the pediatric department saying, “I can’t understand what others are saying or I turn on the TV loudly,” when the first diagnosis of acute otitis media and treatment begins. there is also
• Antihistamines or nasal mucosal bleeding relievers are said to be ineffective in the treatment of acute otitis media.10 and 30.
• When acute otitis media progresses to chronic otitis media, the tympanic membrane is punctured and pus from the middle ear cavity flows into the external auditory meatus through the hole in the eardrum, or complications such as mastitis, osteomyelitis, and meningitis may occur.
Figure 54. Otitis media can cause hearing loss. Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
• When these complications occur, you must be hospitalized and treated with surgery and/or antibiotics.
• The tympanic membrane punctured by acute otitis media usually closes on its own after proper treatment of acute otitis media.
• It is said that severe ear pain caused by acute otitis media is relieved within 1 hour when CO2 laser treatment is used.
• It can be treated with tympanostomy with laser, ventilator insertion, and pus can be drained from the middle ear cavity.
• There is also a study result that it is impossible to prevent the recurrence of acute otitis media with effusion by receiving the basic vaccination with the Streptococcus pneumoniae vaccine.
The following is an example of a question-and-answer question for children and adolescents on the Internet regarding “otitis media”.
Q&A. otitis media
Q. • Your baby is 17 months old.
• When you catch a cold, you often get otitis media. I’ve had a cold 3 times this year, and all 3 of them were due to otitis media.
• The doctor said that if there is a new pneumococcal vaccine, and if you vaccinate it, you can prevent it to some extent. What should I do?
• please answer about my question… A.
• Myung Hee
• Good morning. Thank you for asking a question.
• We can give you a better answer if you have a lot of information, such as your child’s age, gender, past and family medical history, examination findings, and clinical test results. We will respond based on the information you have provided.
■ Bacteria that cause otitis media
• Streptococcus pneumoniae (29.8%) is the most common bacterial causative agent.
• Acute otitis media caused by a streptococcal infection can be prevented to some extent by vaccination with a streptococcal vaccine.
• However, there are many strains of Streptococcus pneumoniae, and the pneumonia vaccine cannot prevent all types of Streptococcus pneumoniae otitis media infection
• Studies have shown that the incidence of acute otitis media is slightly reduced after initiation of vaccination with the Streptococcus pneumoniae vaccine.
• In other words, although vaccination against Streptococcus pneumoniae can slightly reduce the incidence of otitis media, vaccination against Streptococcus pneumoniae cannot prevent all types of Streptococcus pneumoniae, and bacterial infections other than Streptococcus pneumoniae. can cause acute otitis media. • In order to prevent streptococcal otitis media pneumonitis, it is recommended to be vaccinated with the pneumococcal vaccine, as well as receive the pneumococcal vaccine to prevent streptococcal meningitis and pneumonia.
• Otitis media can be caused by one or two of the following types of bacteria.
• Streptococcus pneumoniae (29.8%);
• Buranham ella catalaris (Moraxella catallaris) (11.7%),
• Haemophilus influenzae (20.9%),
• group A beta-hemolytic streptococci (3.1%);
• Staphylococcus aureus (1.6%);
• Pseudomonas erginosa (1.2%),
• Bacteria such as E. coli mainly cause otitis media in children.
• Otitis media can occur when one type of bacteria infects one or both middle ears.
• % in parentheses is the percentage of bacteria that cause otitis media (source – Bluestone CD, Klein JO).
• For reasons and causes of otitis media in children, please refer to information on acute otitis media.
• Viruses or Mycoplasma can also cause acute otitis media, and children of all ages can get otitis media, but the following children are more prone to acute otitis media.
■ Conditions that may predispose you to acute otitis media.
• The younger you are, the less resistant you are to bacterial invasion, and the more likely you are to develop acute otitis media, especially in young children (see p.00 Newborn Otitis Media).
• Abnormally enlarged adenoids can more easily block the entrance to the eustachian tube. Other causes, such as allergic rhinitis, can cause otitis media to be more likely due to blockage of the ear canal. For this reason, children with abnormally enlarged adenoids are more likely to develop otitis media.
• The length of the tube for infants and toddlers is shorter than that for children of school age, adolescents, or adults after infancy. Bacteria from the pharynx or nasal passages of infants and young children can easily pass through the short ear canal and easily enter the middle ear cavity.
• So young children are more prone to otitis media.
• Also, the eustachian tube of infants and young children is thinner than that of adults.
• If you have a cold or other types of viral upper respiratory tract infections, sinusitis (sinusitis), or allergic rhinitis, your ear canal can become easily swollen and blocked.
• At this time, the pressure in the middle ear cavity changes to negative pressure, and the exudate accumulates in the middle ear cavity, and the exudate passes through the ear canal and becomes a good culture medium for bacteria to enter the middle ear cavity. For this reason, otitis media may be more likely to develop.
• Infants who eat artificial nutrition containing milk protein instead of mother’s milk, infants with atopic constitution, and infants with allergic diseases such as bronchial asthma, allergic rhinitis, and atopic dermatitis are susceptible to viral upper respiratory tract infections such as colds. You may be more prone to otitis media when you are sick.
• If one of your biological parents’ siblings has a frequent history of otitis media, other siblings are also more likely to get otitis media.
• Contradictory studies have shown that infants and toddlers are more or less likely to develop otitis media if they suck on a soother. Infants and young children may be more prone to otitis media from other causes.
• See acute otitis media.
• For more information, please consult with the Department of Pediatrics.
• Come back for more questions. Thank you. Lee Sang-won.MD
CONCLUSIONS
Among children 6 to 35 months of age with recurrent acute otitis media, the rate of episodes of acute otitis media during a 2-year period was not significantly lower with tympanostomy-tube placement than with medical management. (Funded by the National Institute on Deafness and Other Communication Disorders and others; ClinicalTrials.gov number, NCT02567825. opens in new tab.) 소스: NEJM 6/2021
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy of Pediatrics
-
drleepediatrics.com제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, harvey grant and robert murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies , Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gerhon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”