급성 부비동염(급성 부비강염/급성 축농증/급성 코곁굴염) Acute paranasal sinusitis(Acute sinusitis)
급성 부비동염(급성 부비강염/급성 축농증/급성 코곁굴염)의 개요와원인
-
상악동, 사골동, 전두동, 접형동이 양쪽에 한 개씩 총 8개의 부비동이 있는 것이 정상이다(그림 8, 9 및 사진 10, 11 참조).
-
각종 병원체가 부비동에 감염되어 생긴 감염병을 부비동염이라고 한다.
-
병원체 말고 항원으로 부비동염이 생길 수 있다.
-
급성 박테리아 부비동염은 소아들에게 흔히 생기는 감염병이다.
-
부비동염은 항생제 치료를 요하는 전 연령층 감염병들 중 다섯 번째로 흔한 감염병이다.
-
항생제치료를 요하는 소아들의 감염병 중 21%가 부비동염이라고 한다(출처; Pediatric Annals 0ctober 2008).
-
부비동에 생긴 염증을 부비동염, 부비강염, 또는 코곁굴염이라 한다.
-
또 부비동염을 비 의료인들은 축농증이라고 부르기로 한다.
-
비강 주위에 있는 동을 부비동, 코곁굴, 또는 부비강이라도 한다.
-
이 부비동 속과 비강 속은 가는 자연 통기관으로 서로 연결되어 있는 것이 정상이다.
-
부비동의 종류와 자녀의 나이에 따라, 태어나서 성인이 될 때까지 부비동의 발육과 성장은 다르다.
|
다음은 “코피가 자주 나요...”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A. 코피가 자주 나요...
Q.
7살 된 남자아이 입니다. 어릴 때부터 감기로 병원을 자기 집 들르다시피 했어요. 5살부터는 소아청소년과에서 이비인후과로 옮겨 다니고 있습니다. 비염이 있어 코가 약해 코피가 날수 있다는 건 알고 있어요. 하지만 너무 자주(한 달에 한 번꼴) 흘려요. 다른 아이들에 비해. (저는 태어나서 한 번도 코피를 흘린 적이 없는데…) 조금 나다 말면 별 걱정이 없을 텐데. 이건 정말 코피인지 알 수 없을 정도로 줄줄 흘러, 보는 사람이 질겁할 정도예요. 병원에서는 별것 아니라고 하지만 제가 보기에는 곁으로 코에 이상이 있을 때 ‘감기가 걸렸다든지‘ 할 경우에는 코피를 안 흘려요. 어린이 집에서는 조금씩 정도밖에는 안 흘린데요. 근데 이상하게도 잠자다 ‘엄마 나 코피나‘할 때 보면 엄청 많이 흘려요. 정말 비염 때문에 다른 아이들보다 자주 코피를 흘리는 걸까요???
A.
- 승원님께
- 안녕하십니까. 질문해 주셔서 감사합니다.
- 자녀의 나이와 성별, 과거 현재 가족의 병력, 증상 징후와 진찰소견, 적절한 임상검사 등의 결과를 종합해서 진단 치료하는 것이 이상적이지만 주신 정보를 참작해서 답변을 드립니다.
- 만일 아드님을 제 소아청소년과로 데리고 오신다면 과거 가족 병력을 들어 보고 알레르기 병력, 성장 발육 과정, 임신 출생 병력, 습관, 그외 더 자세한 병력을 들어보고 머리끝부터 발끝까지 신체검사를 하겠습니다.
- 특히 비경이나 비 내시경으로 비강을 들여다보겠습니다.
- 신체검사에서 피부에 출혈 반점이 없고 비강 속에 별 이상이 없거나 비강 점막 층이 창백해 보이고 눈 밑에 알레르기 샤이너가 있고 과거에 천식이나 알레르기성 비염을 앓았던 병력이 있고 친 부모 형제 재매들에게도 알레르기성 질환이 있는 가족 병력이 있으면 아드님에게 자주 나는 코피는 알레르기성 비염으로 생길 가능성이 가장 많다고 진단하겠습니다.
- 때로는 알레르기성 비염과 축농증이 같이 있는 경우도 많습니다.
- 신체검사의 결과가 정상이고 부모가 아드님의 코피 때문에 걱정을 많이 하시고 세 번 이상 저의 소아청소년과에 상담하러 오시면 CBC 혈액 검사, 출혈의 원인을 알아보기 위해 하는 출혈 스크린 검사(Bleeding screening test)(표23 참조)를 해서 전신 출혈성 질환이 있나 알아보겠습니다.
- 이런 검사는 비교적 간단한 피검사이고 피의 응고가 잘 되는지 알아보는 검사입니다.
- 검사의 결과가 정상이면 이비인후과에 보내서 이비인후과 전문의 의견도 들어보겠습니다.
- 이비인후과 전문의에게 의뢰하겠습니다.
- 의뢰 받은 이비인후과 전문의가 자녀의 코피는 알레르기성 비염으로 난다고 진단을 하고 저에게 아드님을 다시 보내면서 저보고 계속 알레르기성 비염을 치료하라고 하시면 자녀의 알레르기성 비염을 알레르기성 비염을 유발시킬 수 있는 항원 제거나 항원 피함 등 환경 정리 치료방법으로 치료하고 비강 분무용 스테로이드제, 제 2세대 항히스타민제 등으로 치료하라고 저에게 제시하면 저도 이비인후과 전문의 치료방법에 따르겠습니다.
- 자녀의 코피를 치료할 때는 자녀와 부모와 함께 상담해서 그 자녀의 병에 가장 좋은 치료 방법을 물론 선택해서 치료하겠습니다.
- 이상 말씀드린 것을 참고로 해서 치료를 해 보십시오.
- [부모도 반의사가 되어야 한다–소아가정간호백과]-제15권 소아청소년 알레르기 및 면역질환–알레르기성 비염, 제18권 소아청소년 이비인후 질환–코피(비출혈) 등을 참조하시기 바랍니다.
- 그리고 질문이 더 있으시면 다시 연락해 주시기 바랍니다. 감사합니다.이상원 드림
-
상악동은 태어났을 때 이미 생겨 있고,
-
상악동과 사골동은 생후 1~2세에 부비동 X-선 검사 상에 잘 나타날 수 있고,
-
전두동은 생후 2세에서부터 발육되기 시작하고,
-
전두동과 접형동은 생후 5~6세경에 X-선 검사 상에 잘 나타나는 것이 보통이다.
-
급성 부비동염의 99.5%가 바이러스 감염으로 생긴다(출처; Pediatric annals 0ctober 2008).
-
감기 등 바이러스 상기도 염을 일으킨 바이러스가 부비동에 감염되어 바이러스 급성 부비동염이 생길 수 있다. 급성 부비동 염은 세균 감염으로도 생길 수 있다.
표 1. 급성 부비동염 또는 아급성 부비동염을 일으키는 세균의 종류(소아에서)
| 세균의 종류 | 퍼센타일(%) |
| 연쇄상 폐렴구균 (Streptococcus Pneumoniae) | 30 |
| 모락스엘라 캐타라리스 (Moraxella Catarrhalis) | 20 |
| 헤모필러스 인플루엔자 (Haemophilus Influenzae) | 20 |
| 연쇄상 파이오제네스 (Streptococcus Pyogenes) | 4 |
| 그 외 (Others) | 26 |
출처: The Journal of allergy and clinical immunology vol. 99, #6 June 1997, p.840
-
급성 바이러스 부비동염의 대부분은 바이러스 상기도 염이 다 나을 때 부비동염도 동시에 낫는 것이 보통이다.
-
또 감기나 다른 종류의 바이러스 상기도 염을 앓을 때 폐렴연쇄상구균이나 헤모필러스 인플루엔자균 감염으로 급성 박테리아 부비동염이 생길 수 있고,
-
또는 드물게 포도상구균이나 A군 연구균 감염에 의해서 급성 부비동염이 이차 세균 감염으로 생길 수 있다.
-
또 드물게는 부비동에 진균 감염으로 진균성 부비동염(충농증)이 생길 수 있다.
-
이런 종류의 박테리아가 부비동에 1차로 감염 되어 급성 박테리아 부비동염이 생길 수 있다.
-
알레르기 진균 부비동염(Allergic fungal sinusitis)도 드물게 생길 수 있다.
-
S. milleri 연구균 감염에 의해서 급성 부비동염이 생길 수 있다.
-
메치실린(Methicillin) 항생제 내성이 있는 황색 포도상구균(MRSA)의 감염으로 급성 부비동염이 생길 수 있다.
-
남여 노소 모든 연령층 누구든지 급성 박테리아 부비동염에 걸릴 수 있다.
-
알레르기 비염, 기관지 천식, 아토피성 피부염, 다른 종류의 알레르기 질환이나 아토피성 체질을 가지고 있는 아이들에게 급성 부비동염이 더 잘 생길 수 있다.
-
부비동염 참조
-
알레르기 비염 참조
재발성 부비동염을 잘 일으키게 하는 질병들
- 부비동 섬모 증후군,
- IgA 면역 글로불린 결핍증,
- 비용(폴립),
- 비중격 기형,
- 비 종양,
- 비강 이물,
- 아데노이드 비대,
- 낭포성 섬유증,
- 기관지 확장증,
- 국소 치료용 비강점막 충혈완화제 과도 사용,
- 마약 사용,
- 알레르기 비염,
- 간접 흡연,
- 수영과 다이빙,
- 후천성 면역 결핍 증후군,
- 그 외
급성 부비동염(급성 부비강염/ 급성 축농증/ 급성 코곁굴염)의 증상 징후
-
급성 부비동염의 증상 징후는 다양하다.
-
환아의 나이, 급성 부비동염을 일으킨 병원체의 종류, 급성 부비동염이 생긴 부비동의 종류, 급성 부비동염이 있을 때 같이 있는 동반 병(동반 질환)의 종류에 따라 증상 징후가 다르다.
-
급성 부비동염의 증상 징후는 감기의 증상 징후와 거의 비슷할 수 있다.
-
미열이 날 수 있고 고열이 날 수 있다.
-
학령기 전 유아들은 두통을 호소할 수 있다.
-
식욕이 감소되기도 하고 식욕이 상실될 수 있다.
-
어려서 말로 표현을 잘 할 수 없는 영유아에게 급성 부비동염이 생기면 보채고 울 수 있고 잠도 잘 자지 못한다.
-
급성 부비동염이 생긴 부비동이 있는 부위가 아프고, 그 부비동이 있는 부위에 압박감이 생기고, 드물게는 그 부위가 부을 수 있고 손으로 누르면 압통이 있다.
-
눈과 콧등의 사이에 있는 사골동(사진 112, 113 참조)에 급성 부비동이 생기면 안와 주위 봉소염([부모도 반의사가 되어야 한다–소아가정간호백과]-제19권 소아 청소년 안과 질환–안와위 봉소염 참조)이 생길 수 있고,
-
그 쪽 안구 주위 부종이 생기거나 머리가 아플 수 있다.
-
급성 부비동은 없이 감기만 앓을 때 나는 콧물의 대부분은 맑은 점액성이다.
-
감기는 7~14일 이상 계속 되지 않는 것이 보통이다.
-
알레르기 비염을 앓을 때는 물과 같이 맑은 콧물이 나며 7~14일 이상 계속 될 수 있다.
-
급성 부비동염이 있을 때는 콧물 색은 누렇거나, 푸르스름하고 짙은 것이 보통이다.
-
코에서 냄새가 날 수 있다.
-
냄새를 잘 맡지 못할 수 있다.
-
드물게는 급성 부비동염이 있지만 콧물은 조금도 나지 않을 수 있다.
-
급성 부비동염이 있으면 코가 자주 막히고 기침도 조금 할 수 있다.
-
특히 밤에 자다가 기침을 더 많이 한다.
-
급성 부비동염으로 기침을 하기보다 천식 등 동반 질병으로 기침할 때가 많다.
-
기관지 천식이 있는 아이들의 대부분은 밤에 자다가 수면 유발성 천식이 생겨 그로 인해 기침을 많이 한다([부모도 반의사가 되어야 한다–소아가정간호백과]-제15권 소아 청소년 알레르기 및 면역질환–야간 수변 유발성 기관지 천식 참조).
-
때로는 이 두 가지 병이 같이 있을 수 있다.
-
아이가 자다가 기침할 때는 이 두 가지 병이 같이 있는지 알아봐야 한다.
-
참고로, 부비동염만 있을 때 그 부비동염 자체로 밤에 자다가 기침을 거의 하지 않는 것이 보통이다.
-
급성 박테리아 부비동염을 조기에 적절히 치하지 않으면 급성 부비동염이 만성 부비동염으로 된다.
-
학령기나 사춘기 아이들이 급성 부비동염을 앓을 때 보통 이상으로 피로하거나 정신집중이 잘 안되어 주의력 결핍장애가 생기고 과도 활동 장애도 생길 수 있다.
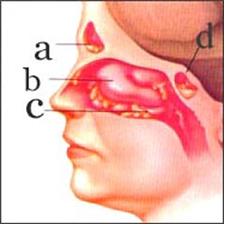
그림 110. 급성 박테리아 부비동염.
a-전두동, b-비강, c-부비동염으로 생긴 고름, d-접형동.
출처; Used with permission from Schering corporation, kenilworth, NJ, USA와 소아가정간호백과
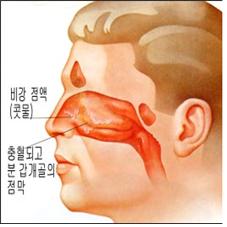
그림 111. 감기 등 바이러스 급성 비염만 있을 때 비강.
출처; Schering Corporation, Kenilworth, NJ, USA와 소아가정간호백과
급성 부비동염(급성 부비강염/급성 축농증/급성 코곁굴염)의 진단
-
특별한 검사를 하지 않고 병력, 증상 징후와 진찰소견 등을 종합하고 임상적 경험을 토대로 부비동염을 진단하는 경우가 보통이다.
-
비경으로 비강 속을 진찰해 보면, 비강 점막층이 붓고 비갑개에 점액과 고름이 있을 수 있다(그림 110 참조).
-
비강 점막층이나 부비동의 점막층에서 나온 비강 내 고름이나 콧물을 채취해서 그 피 검물로 세균 배양 검사를 해 원인 되는 박테리아의 종류를 알아볼 수 있다.
-
그러나 비강 점막층에서 채취한 세균검사용 피 검물로 세균검사를 한 결과가 진단 상 신빙성이 별로 없을 수 있다.
-
부비동 X-선 사진 검사, CT 스캔 검사, MRI 검사, 초음파 검사 등으로 진단할 수 있다.
-
그 중 부비동 CT 스캔 검사가 부비동 염을 진단하는데 더 가치가 있다.
-
그러나 영유아의 부비동 염을 진단하는데 CT 스캔 검사도 별 가치가 없다.
-
비강 내 내시경으로 진단할 수 있다.
급성 부비동염(급성 부비강염/급성 축농증/급성 코곁굴염)의 합병증
-
급성 박테리아 부비동염의 합병증 중 가장 흔한 합병증은 안와 감염병이다.
-
챈들러의 합병증 분류(Chandler Classification)에 의하면 안와 감염병을 5가지 그룹으로 분류한다.
-
안구농양,
-
안구골막하 농양,
-
안구 주위염,
-
실명 등이 안와 감염으로 생길 수 있다.
-
경막외 농양,
-
경막하 농양,
-
뇌막염,
-
뇌농양,
-
뇌염,
-
두골 골염,
-
해면 정맥동 혈전증(Cavernous sinus Thrombosis),
-
점액류,
-
비용(비강 폴립),
-
종양,
-
패혈증 등의 합병증이 부비동염이 있을 때 생길 수 있다.
-
이런 합병증은 수술치료도 한다.
-
출처: The Journal of allergy and clinical immunology vol. 99, #6 June 1997, p.842.
급성 부비동염(급성 부비강염/급성 축농증/급성 코곁굴염)의 치료
-
급성 부비동염이 생긴 부비동의 종류, 원인이 되는 세균의 종류, 환아의 나이, 합병증의 유무, 부비동염을 일으킨 다른 원인에 따라 치료가 다르다.
-
급성 부비동염과 감기가 함께 있을 때는 감기로 생긴 증상 징후에 따라 감기를 대증치료하고 급성 박테리아 부비동염은 적절한 항생제로 치료한다.
-
비강 점막층 충혈은 비강 점막 충혈 완화 점비제(적제), 분무제, 경구용 시럽이나 알약 등으로 치료한다.
-
페닐에프린은 비강 점막 충혈 완화제의 일종이다.
-
페닐에프린 비 점비제 등은 비강 속에 넣어 비강 점막층 모세 혈관 충혈을 수축시키는 작용이 다.
-
비강 내에 넣어 비강 점막 충혈을 완화 시킬 수 있는 페닐에프린 코 점비제로 치료할 때는 3일 이상 치료하지 않는 것이 보통이다.
-
경구용 슈도에페드린 등 비강 점막 충혈 완화제로 부비동염을 치료하기도 한다.
-
슈도에페드린 등 경구용 비강 점막 충혈 완화제로 부비동염을 치료할 때는 콧물이 더 이상 나오지 않고 비강 점막 충혈이 완화되어 비강이 숨쉬기에 좋게 확 뚫릴 때까지 계속 복용할 수 있다.
-
부비동염을 비강 점막 충혈 완화제 치료에 관해 찬반이 있으므로 의사의 지시에 따라야 한다.
-
부비동염으로 열이 나거나 머리가 아플 때는 타이레놀 등 해열 진통제로 해열 진통시킨다.
소아 급성 박테리아 부비동염은 다음 여러 종류의 항생제들 중 한 종류나 두 종류를 선택해 치료한다.
-
Amoxicillin 아목시실린,
-
Amoxicillin/clavulamic acid 오그멘틴,
-
Erythromycin/sulfioxazole,
-
Sulfamethoxazole/trimethoprim,
-
Cefaclor,
-
Cefuroxime axetil,
-
Cefprozil,
-
Cefpodoxime proxetil,
-
Loracarbef,
-
Clarithromycin,
-
Clindamycin,
-
그 외 다른 종류의 항생제들 중 한 가지를 골라 2~6주간 치료하는 것이 보통이다.
-
고열이 나고 급성 부비동염이 심할 때는 병원 입원해 항생제 정맥주사로 치료 한다.
-
때로는 항생제 치료와 비강 속 코르티코스테로이드제 분무로 치료 한다.
-
생리 식염수 5 방울로 좌우 양쪽 비강 속에 하루 4번, 10일 동안 치료하면 치료효과가 좋다고 한다. 물론, 필요에 따라 외과적 수술치료도 한다.
|
2012년 미 감염병학회 성인 급성 부비동염 치료 가이드라인 다음 1~5의 증상이나 조건이 있으면 바이러스성 비 부비동염이라고 진단하기 보다 박테리아성 부비동염이 있다고 진단한다
박테리아성 비 부비동염은 다음과 같이 치료한다.
|
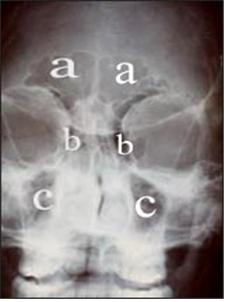
사진 112. 부비동 X-선 사진.
a-전두동, b-사골동, c-상악동.
Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
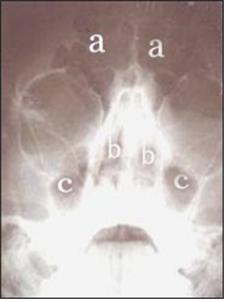
사진 113. 부비동 X-선 사진.
a-전두동, b-사골동, c-상악동.
Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
|
다음은“알레르기 비염, 부비동염 재발”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
- Q&A. 알레르기 비염 부비동염 재발
- Q.
- 아래 글에 몇 번 아이 두통 때문에 문의 드렸던 6세 아이 엄마입니다.
- 아이가 5일간 새벽녘이나 잠 깰 때 머리아프다고 하여 소아청소년과 에서 맥박도 재고 안과에서 안압도 쟀지만 다 정상으로 나왔었어요.
- 그런데 그런 뒤에 아이가 잠에서 깰 때 보니 한쪽 코가 막히고 코 속살이 부어있었어요.
- 그래서 소아청소년과 선생님은 휴가 중이라 이비인후과에 가보았더니 글쎄 그만 그사이에 부비동염 이래네요.
- 소아청소년과 에서 약을 그동안 기침 때문에 항생제 오그멘틴 듀오랑 스테로이드제 신티손을 계속 먹어 왔는데 먹는 도중에 머리가 아팠었거든요.
- 그런데 약을 떼자 머리는 안 아파왔고 약 뗀지 3일 만에 코가 이상하여 가보니 콧속에 노란 코가 가득 찼다고 부비동염 이라고 하네요. 어떻게 이리 빨리 재발을 할 수가 있는지요?
- 약을 먹는 중에도 감기가 오면 바로 재발하는 건가요?
- 그 동안 3주 정도는 코가 깨끗했었거든요. 3개월 1주간이나 부비동염 치료를 했는데 약 뗀지 3일 만에 다시 부비동염 이라니 기가 막혀서요.
- 그리고 이비인후과에서 자디텐이라는 약 때문에 아이가 부비동염 이 된 것 같다고 해요. 그 약이 코를 못나오게 꽉 잡아주니까 배출이 안 되어 그런 거라고요.
- 우리아이는 부비동염 약을 떼고 자디텐이라는 예방약만 날마다 두 번 먹고 있었거든요.
- 소아청소년과 선생님 말씀을 따르자니 그렇고 이빈후과에만 다니자니 아이 전반적인 건강이 불안하고..어떡하면 좋지요? 게다가 이빈후과에서 준 약이 설파제와 소아용 루리드 현탁액정과 비충혈제거제인 슈….(이름이 잘 생각 안 나서) 에요.
- 전에 다 먹어봤던 약이라 효과가 있을지 해서요. 어떡하면 좋겠습니까? 소아청소년과 선생님 휴가가 끝나면 다시 소아청소년과 로 가야할까요?
A.
- 순희님
- 안녕하세요. 또 좋은 질문을 해주셔 감사합니다. 자녀의 나이 , 성별, 과거 병력, 진찰소견 등의 자세한 정보를 주셔 감사합니다. 저도 걱정하시는 어머님을 어느 정도 이해할 수 있습니다.
- 그 동안 의사께서 직접 진찰 진단 치료하셨는데 제가 도움 될 말씀을 드릴 수 있을 까 우선 걱정부터 합니다.
- 제가 아드님을 치료하는 단골 청소년과 의사라면 다음과 같이 치료해 볼 수 있다고 생각합니다.
- 전에도 말씀드린 바와 같이 제 생각으로 자녀는 아토피성 체질을 가진 것 같습니다.
- 아토피성 체질을 가진 아이들의 대부분은
- 알레르기 비염,
- 부비동염(축농증),
- 크루프,
- 기관지 천식,
- 아토피성 피부염,
- 알레르기 결막염,
- 두통,
- 어지럼증,
- 가성빈혈,
- 알레르기 샤이너,
- 우유 알레르기,
- 긴장성 피로 증후군,
- 곤충 알레르기 등
- 여러 종류의 알레르기 질환과 그로 인하여 징후 증상이 생길 수 있습니다.
- 사실은 이런 알레르기 질환을 알게 모르게 앓고 있는 사람들의 대부분은 그런 알레르기 질환을 가지고 있는지 본인도 모르고 사는 경우가 아주 많습니다.
- 저 역시도 미국에 와서 의학 공부를 더 하기 전에 그런 문제로 많이 고생한 사람들 중 한 사람입니다.
- 불행하게도 알레르기 질환을 완치시키는 특효약이 없습니다. 예방적 치료를 하는 데 주력을 두어야 합니다.
- 걱정하지 마시고 예방적 치료를 잘 하시고 그때그때 치료를 잘하시면 그렇게 큰 건강 문제가 생기지 않습니다.
- 요즘 그런 알레르기 병을 예방적 치료를 하는데 많은 종류의 약물들이 있고 부작용도 적고 예방적 치료도 잘 됩니다.
- 첫째로 부비동염의 원인은 아주 많다는 것을 말씀드리고 싶습니다.
- 예측할 수 없이 재발될 수 있습니다.
- 학령기 아이들이 감기를 연간 8번 정도 앓는 것이 보통이지만
- 같은 연구에 의하면 연간 22번 정도 앓는 아이들도 있습니다.
- 감기 들면 그 감기를 일으킨 바이러스가 비강 점막층과 인두 점막층에 감염병을 일으키고 부비동에 있는 점막층에 감염병을 일으키는 것이 보통입니다.
- 이 때 2차 세균 감염이 생기지 않는 한 감기는 자연적으로 나으면서 바이러스성 부비동염도 자연히 나을 수 있습니다.
- 만일 감기로 인한 바이러스성 부비동염에 이차 세균(박테리아) 감염이 생기면 박테리아 부비동염이 생기는 것입니다.
- 이때는 감기만 있을 때의 증상 징후 보다 더 심한 증상 징후가 생기고 콧물이 더 짙고 더 노랗고 때로는 푸르스름해 집니다.
- 두통, 피로, 열, 부비동염이 있는 부위에 압통이 생길 수 있습니다.
- 그러나 어떤 때는 그런 증상 징후가 거의 생기지 않을 수 있습니다.
- 아시겠지만 부비동염의 진단은 증상 징후와 과거, 현재의 병력 등을 참고해서 주로 진단하는 때가 많기 때문에 의사들도 때로는 오진 할 수 있습니다.
- 일반적으로 부비동 X-선 사진이나 CT 스캔 검사 또는 MRI 사진 검사를 하지 않고 세균검사도 않고 임상 경험에 비추어 추정 진단하고 그에 의해서 치료하는 경우가 더 많습니다.
- 감기에 걸리지 않았을 때도 알레르기 비염이 있는 아이들의 대부분의 경우, 비강 내 점막층도 붓고 부비동 점막층도 함께 부을 수 있습니다.
- 때에 따라 박테리아나 바이러스 또는 곰팡이가 부비동 속에 감염되면 부비동염이 생길 수 있습니다.
- 어떤 세균이 부비동염을 일으켰느냐에 따라서 그 부비동염을 앓는 자녀의 나이와 알레르기 비염이 있느냐에 따라 급성 또는 만성이냐에 따라, 또는 다른 조건에 따라 부비동염의 증상 징후와 중증도, 치료 예후 등이 아주 다릅니다.
- 부비동염이 자주 생기면 때로는 면역 기능이 정상인지 비정상인지 알아보고 또 비강과 상하기도 점막층의 섬모 기능이 정상인지도 알아보아야 할 때가 있습니다.
- 이런 복잡한 의학지식을 염두에 두시고 부비동염(축농증)을 항생제와 다른 약물로 적절히 치료해도 잘 낫지 않아 부비동염은 수술로 치료해야 할 때가 있습니다.
- 항생제로 치료할 때는 보통 10-14일 동안 치료할 때도 있고 때로는 6주 정도 치료할 때도 있습니다.
- 그렇게 치료해도 재발될 수 있습니다. 그 재발하는 것을 예방하기 위해 예방적 치료를 잘 해도 재발되는 경우가 있습니다.
- 소아들이 부비동염 등을 앓고 있는 것 같으면 위에서 설명한 바와 같이 부비동염의 원인은 알레르기, 면역기능, 기도 섬모기능, 성장발육 등과 관련되어 있기 때문에 1차적으로 우선 소아청소년과에서 진단 치료받는 것이 이상적입니다.
- 그러나 경우에 따라 물론 소아청소년과 이외 다른 과 전문의의, 특히 이비인후 전문의의 치료를 받을 수 있습니다.
- 잘 치료되지 않는 부비동염이 있으면 이비인후과 전문의, 소아 알레르기와 면역 전문의, 소아 감염병 전문의, 소아 호흡기 전문의 등 여러 특수 전문의들이 서로 의뢰해서 팀 치료를 할 때도 있습니다.
- 이런 치료를 받을 때는 가능한 한 단골 소아청소년과 의사의 판단에 따라 적절한 이비인후과 전문의나 다른 특수 전문의에게 의뢰해서 그 특수 전문의가 한 팀이 되어 치료하면 가장 이상적인 치료방법이 될 것입니다.
- 이렇게 치료를 할 때는 각 전문의의 의견을 서로 듣고 가장 적절한 방법으로 치료할 수 있기 때문에 단골 소아청소년과 전문의와 다른 특수 전문의가 거의 동일한 약으로 치료할 수 있습니다.
- 그러나 이런 방법으로 치료를 할 때는 의료비가 많이 들고 그렇게 치료할 수 있는 사회적 의료행정 조건들이 구비되어야 합니다.
- 일반적으로 급성 부비동 염을 치료할 때 비강 속에서 얻은 콧물 피검물로 그람 염색 세균 현미경 검사와 세균배양 검사를 하지 않고 임상적 경험에서 얻을 정보를 토대로 항생제로 선택하여 치료하지만 때로는 전신 증상을 나타내는 부비동염, 특히 심한 박테리아 부비동염이나 치료가 잘 되지 않는 부비동염을 앓을 때는 비강 속 점막에서 얻은 피검물이나 부비동염이 있는 부비동 속에서 주사 바늘 천자로 얻은 피검물로 세균검사를 할 수 있습니다.
- 일반적으로 어떤 종류의 세균이 부비동염을 일으키는지 알아보기 위해서 세균배양검사를 통상적으로 하는 것은 별 가치가 없다고 합니다.
- 때로는 그런 세균 검사를 해서 어떤 세균이 부비동염을 일으키나 알아보고 그 세균으로 감염된 부비동 염을 치료할 수 있는 항균제 감수성 검사도 해서 가장 적절한 항생제로 부비동염을 치료하는 것이 가장 이상적일 때도 있습니다.
- 세균검사를 하지 않고 설파제인 셉트라(Septra)나 오그멘틴(Augmentin) 등과 항히스타민제나 비강 점막 충혈 완화제로 비강 점막 모세혈관을 수축시켜 치료 하고, 또 코르티코스테로이드제 비강 분무제 등으로 부비동염을 치료할 수 있습니다.
- 그리고 백혈구기능, 상기도 점막 기능, 면역 기능 등이 정상인지 알아보아야 할 때도 있습니다.
- 알레르기 비염이나 부비동염 또는 기관지 천식 등이 있으면 그런 알레르기 질환이 생기지 않게 우유 등 알레르기 질환을 잘 일으킬 수 있는 음식물, 환경오염, 집 먼지 좀 진드기, 스트레스, 애완동물, 약물, 흡연 등에 노출되지 않도록 환경 관리를 잘 해서 알레르기를 예방하는 것도 상당히 중요하고 클라리틴(Claritin-Loratadine) 등 2세대 항히스타민제 및, 또는 크로몰린 소듐(Cromolyn sodium) 비강 분무제, 또는 코르티코스테로이드제 비강 문무제 등으로 치료 및 예방하고 적절한 항생제로 치료할 수 있습니다.
- 이런 치료를 할 때 전에 말씀드린바와 같이 단골 소아청소년과 전문의의 치료를 받는 것이 적절하고 필요에 따라 소아 알레르기 전문의나 이비인후과 전문의에게 의뢰해서 함께 치료할 수 있습니다.
- 이런 치료방법은 어디까지나 그렇게 치료해 볼 수 있다는 것을 말씀드리는 것입니다.
- 진단 치료를 할 때는 어디까지나 자녀의 의사의 판단에 따라(자녀가 성숙했으면) 약의 형태를 선택하는 것도 중요합니다.
- 약의 종류, 용량, 쓰는 기간 등을 의사와 상의해서 결정해야 합니다.
- [부모도 반의사가 되어야 한다–소아가정간호백과]-제15권 소아 청소년 알레르기 및 자가 면역질환을 많이 읽어보시면 거기에서 의문점에 관한 정보와 답변을 많이 얻을 수 있을 것입니다. 특히 부비동염, 천식, 알레르기 비염, 알레르기를 일으키는 인자, 항원 등에 대해서도 많이 읽어보시기 바랍니다.
- 알레르기 질환을 효과적으로 잘 치료하기 위해서는 부모들이 1차적 책임을 지고 부모가 적극적으로 동참해야 한다는 것을 다시 말씀드리고 싶습니다.
- 문제가 계속 되면 소아청소년과에서 계속 진찰 진단을 받으시고 그 문제에 관해 상담하시기 바랍니다. 질문이 더 있으면 또 방문하세요. 감사합니다. 이상원 드림
Acute paranasal sinusitis (Acute sinusitis/Acute sinusitis/Acute sinusitis) 급성 부비동염(급성 부비강염/급성 축농증/급성 코곁굴염)
Overview and causes of acute sinusitis (acute sinusitis/acute sinusitis/acute sinusitis)
• It is normal to have a total of 8 sinuses, one on each side of the maxillary, ethmoid, frontal, and sphenoid sinuses (see Figures 8 and 9 and Figures 10 and 11).
• An infectious disease caused by infection of the sinuses by various pathogens is called sinusitis.
• Sinusitis can be caused by antigens other than pathogens.
• Acute bacterial sinusitis is a common infectious disease in children.
• Sinusitis is the fifth most common infectious disease among all age groups requiring antibiotic treatment.
• Sinusitis accounts for 21% of infectious diseases in children requiring antibiotic treatment (source: Pediatric Annals 0ctober 2008).
• Inflammation of the sinuses is called sinusitis, sinusitis, or paranasal sinusitis.
• We also decided to call sinusitis sinusitis by non-medical practitioners.
• The sinuses around the nasal passages are also called sinuses, paranasal sinuses, or sinuses.
• It is normal for these sinuses and nasal passages to be interconnected by a thin natural vent.
• Sinus development and growth vary from birth to adulthood, depending on the type of sinus and the age of the child.
The following is an example of a Q&A on health counseling for children and adolescents on the Internet about “I often have nosebleeds…”.
Q&A.
I have frequent nosebleeds…
Q.
He is a 7 year old boy. Ever since I was little, I used to go to the hospital for a cold. From the age of 5, he has been transferred from the Department of Pediatrics to the Department of Otolaryngology. I know that I have rhinitis and my nose is weak and can cause nosebleeds. But too often (about once a month). compared to other children. (I’ve never had a nosebleed since I was born…) If it’s a little bit better, I wouldn’t worry too much. It flows so much that it’s hard to tell if it’s really a nosebleed, to the point that people who see it are terrified. The hospital says it’s not a big deal, but in my opinion, when there’s something wrong with your nose, if you say you have a cold, you don’t bleed nosebleeds. In the nursery, I only shed a little bit. But strangely, when I see ‘Mom, I have a nosebleed’ while sleeping, I shed a lot. Do you really have nosebleeds more often than other children because of rhinitis???
A.
• To the crew
• Hello. Thanks for asking.
• Although it is ideal to diagnose and treat the child’s age and gender, past and present family history, symptom signs and findings, and appropriate clinical examination results, we will provide an answer based on the information you have provided.
• If you bring your child to my pediatrics department, we will take a family history, allergy history, growth and development, pregnancy and birth history, habits, more detailed medical history, and a head-to-toe physical examination.
• We will look into the nasal cavity, especially with a rhinoscopic or nasal endoscope.
• On physical examination, there are no bleeding spots on the skin, there are no abnormalities in the nasal passages, the nasal mucosa layer is pale, there is an allergy shiner under the eyes, there is a history of asthma or allergic rhinitis in the past, and the biological parents are also allergic If you have a family history of the disease, I will diagnose that your child’s frequent nosebleeds are most likely caused by allergic rhinitis.
• Occasionally, allergic rhinitis and sinusitis coexist.
• If the results of the physical examination are normal and the parents are worried about their child’s nosebleeds and come to my pediatrician for consultation three or more times, a CBC blood test and a bleeding screening test to determine the cause of bleeding ( See Table 23) to see if there is a systemic hemorrhagic disease.
• This test is a relatively simple blood test and checks to see if the blood clots well.
• If the test result is normal, we will send it to the otolaryngologist to hear the opinion of the otolaryngologist.
• Referral to an otolaryngologist.
• If the referred otolaryngologist diagnoses that your child’s nosebleeds are caused by allergic rhinitis and sends me back to my child and tells me to continue to treat the allergic rhinitis, the child’s allergic rhinitis is an antigen that can cause allergic rhinitis. If you suggest to me to treat with environmental cleanup treatment methods such as removal or antigen avoidance, and to treat with nasal spray steroids and second-generation antihistamines, I will follow the treatment method of the otolaryngologist.
• When treating your child’s nosebleeds, we will consult with the child and parents and of course choose the best treatment method for the child’s illness. • Try treatment with reference to the above.
• Please refer to www.drleepediatrics.com- Volume 15 Children’s Allergy and Immune Diseases – Allergic Rhinitis, Volume 18 Children’s Otolaryngology – Nosebleeds
• And if you have more questions, please feel free to contact us. Thank you. Lee Sang-won
• The maxillary sinuses are already formed at birth,
• The maxillary sinuses and ethmoid sinuses can be seen well on x-rays of the sinuses at 1 to 2 years of age,
• The frontal sinuses begin to develop from the age of 2, • The frontal and sphenoid sinuses usually show up well on X-rays around the age of 5-6 years. • Viral infection accounts for 99.5% of acute sinusitis (source: Pediatric annals 0ctober 2008). • Viruses that cause viral upper respiratory tract infections such as colds can infect the sinuses and cause viral acute sinusitis. Acute sinusitis can also be caused by a bacterial infection.
Table 1. Types of bacteria that cause acute or subacute sinusitis (in children)
표 1. 급성 부비동염 또는 아급성 부비동염을 일으키는 세균의 종류(소아에서)
| Bacteria Type 세균의 종류 | Percentile (%)퍼센타(%) |
| 연쇄상 폐렴구균 (Streptococcus Pneumoniae) | 30 |
| 모락스엘라 캐타라리스 (Moraxella Catarrhalis) | 20 |
| 헤모필러스 인플루엔자 (Haemophilus Influenzae) | 20 |
| 연쇄상 파이오제네스 (Streptococcus Pyogenes) | 4 |
| 그 외 (Others) | 26 |
Source: The Journal of allergy and clinical immunology vol. 99, #6 June 1997, p.840
• In most cases of acute viral sinusitis, it is common for sinusitis to heal at the same time when viral upper respiratory tract infection is resolved.
• Also, when you have a cold or other viral upper respiratory tract infections, you may develop acute bacterial sinusitis due to infection with Streptococcus pneumoniae or Haemophilus influenzae.
• Or, rarely, acute sinusitis can be caused by secondary bacterial infection due to infection with staphylococcus or group A research bacteria.
• In rare cases, a fungal infection of the sinuses can result in fungal sinusitis (appysis).
• A primary infection of the sinuses with this type of bacteria can lead to acute bacterial sinusitis.
• Allergic fungal sinusitis is rare.
• Acute sinusitis can be caused by S. milleri research bacteria infection.
• Infection with methicillin-resistant Staphylococcus aureus (MRSA) can cause acute sinusitis.
• Acute bacterial sinusitis can occur to anyone of any age, young or old.
• Children with allergic rhinitis, bronchial asthma, atopic dermatitis, other types of allergic disease or atopic constitution are more likely to develop acute sinusitis.
• See Sinusitis
• See Allergic Rhinitis
Diseases that predispose to recurrent sinusitis
1. Sinus Ciliary Syndrome,
2. IgA immunoglobulin deficiency,
3. Cost (polyps),
4. septal malformation,
5. Non-tumor,
6. Nasal foreign body;
7. Adenoid hypertrophy,
8. Cystic Fibrosis,
9. bronchiectasis,
10. Excessive use of nasal mucosal decongestants for topical treatment;
11. drug use;
12. Allergic rhinitis,
13. Secondhand smoke;
14. Swimming and diving;
15. Acquired Immunodeficiency Syndrome,
16. Others
Signs, symptoms of acute sinusitis (acute sinusitis/acute sinusitis/acute sinusitis)
• Symptoms of acute sinusitis are varied.
• Symptoms differ depending on the child’s age, the type of pathogen that caused acute sinusitis, the type of sinus that caused acute sinusitis, and the type of comorbidity (comorbidity) associated with acute sinusitis.
• The symptoms of acute sinusitis may closely resemble those of a cold.
• You may have a low fever and a high fever.
• Preschool children may complain of headaches.
• You may have decreased appetite and may even lose your appetite. • Acute sinusitis in infants and young children who are unable to express themselves in words may cause irritability, crying, and difficulty sleeping.
• In acute sinusitis, the sinus area is painful, there is a feeling of pressure in the sinus area, and in rare cases, the area may be swollen and tender when pressed with the hand.
• If acute sinus occurs in the ethmoid sinus between the eye and the bridge of the nose (refer to photos 112 and 113), periorbital cellulitis see) may occur.
• There may be swelling around the eyeball on that side or a headache.
• Most of the runny nose when you have a cold without acute sinus is clear mucus. • A cold usually does not last more than 7 to 14 days.
• When you have allergic rhinitis, you have a runny nose that is clear like water, and it may last for 7 to 14 days or more.
• In acute sinusitis, the color of the runny nose is usually yellow, bluish and dark.
• Your nose may smell.
• You may not be able to smell well.
• Rarely, there is acute sinusitis, but no runny nose.
• If you have acute sinusitis, you may have frequent stuffy nose and a slight cough. • Coughing more, especially at night.
• More often than not coughing with acute sinusitis, coughing with accompanying diseases such as asthma.
• Most children with bronchial asthma develop sleep-induced asthma while sleeping at night and cough a lot as a result,www.drleepediatrics.com – Vol. See also water-induced bronchial asthma).
• Sometimes these two diseases can coexist.
• If your child coughs while sleeping, check to see if these two diseases are present.
• For reference, when there is only sinusitis, it is normal to cough at night due to sinusitis itself.
• If acute bacterial sinusitis is not treated early and adequately, acute sinusitis becomes chronic sinusitis. • When school-age or adolescent children suffer from acute sinusitis, attention deficit disorder and hyperactivity disorder may occur due to abnormally fatigued or troubled mind.
Figure 110. Acute bacterial sinusitis.
• a-frontal sinuses, b-nasal sinuses, c-sinusitis-induced pus, d-sphenoid sinuses.
• source; Used with permission from Schering corporation, kenilworth, NJ, USA and Encyclopedia of Pediatric and Family Nursing
• Figure 111. Nasal sinus with only viral acute rhinitis, such as a cold.
• source; Schering Corporation, Kenilworth, NJ, USA and the Encyclopedia of Pediatric and Family Nursing
• Diagnosis of acute sinusitis (acute sinusitis/acute sinusitis/acute sinusitis) • It is common to diagnose sinusitis based on clinical experience by synthesizing the medical history, symptom signs, and examination findings without special examination.
• When examining the nasal passages through the nasal passages, the nasal mucosa may swell and there may be mucus and pus in the turbinate (see Figure 110).
• It is possible to identify the causative bacteria by collecting pus or mucus in the nasal cavity from the nasal mucosa or the mucosal layer of the sinuses and performing a bacterial culture test with the blood sample.
• However, the results of bacteriological tests with blood samples collected from the nasal mucosa may not be very reliable in diagnosis.
• It can be diagnosed by sinus X-ray examination, CT scan examination, MRI examination, and ultrasound examination.
• Among them, sinus CT scan is more valuable in diagnosing sinusitis. • However, CT scans are of little value in diagnosing sinusitis in infants and young children.
• Diagnosis can be made by intranasal endoscopy.
• Complications of acute sinusitis (acute sinusitis/acute sinusitis/acute sinusitis)
• The most common complication of acute bacterial sinusitis is orbital infection.
• According to Chandler’s classification of complications, orbital infections are classified into five groups.
• eye abscess;
• subperiosteal abscess;
• periophthalmitis;
• Blindness can be caused by orbital infection.
• epidural abscesses;
• subdural abscess;
• meningitis;
• brain abscess;
• Encephalitis;
• Osteoarthritis of the skull;
• Cavernous sinus Thrombosis;
• mucus;
• cost (nasal polyps);
• tumors;
• Complications such as sepsis may occur when sinusitis is present.
• These complications can also be treated surgically.
• Source: The Journal of allergy and clinical immunology vol. 99, #6 June 1997, p.842.
• Treatment of acute sinusitis (acute sinusitis/acute sinusitis/acute sinusitis)
• Treatment differs depending on the type of sinus causing acute sinusitis, the type of causative bacteria, the age of the child, the presence of complications, and other causes of sinusitis.
• When acute sinusitis and cold coexist, treat the cold symptomatically according to the symptoms and signs caused by the cold, and treat acute bacterial sinusitis with appropriate antibiotics.
• Nasal mucosal congestion is treated with nasal mucosal decongestant nasal drops (red drops), sprays, oral syrups or tablets.
• Phenylephrine is a type of nasal mucosal decongestant.
• Phenylephrine nasal nasal drops are put into the nasal passages to constrict the nasal mucosal capillary congestion.
• When treated with phenylephrine nasal nasal drops, which can be placed in the nasal cavity to relieve nasal mucosal congestion, it is usually not recommended for more than 3 days.
• Sinusitis is sometimes treated with nasal mucosal decongestants, such as oral pseudoephedrine.
• When treating sinusitis with an oral nasal decongestant such as pseudoephedrine, you can continue to take it until the nasal passages are cleared for breathing because the nasal mucosal congestion is relieved and the runny nose is no longer produced.
• There are pros and cons to treating sinusitis with nasal mucosal decongestants, so follow your doctor’s instructions.
• If you have a fever or a headache due to sinusitis, use an antipyretic analgesic such as Tylenol to relieve fever.
Acute bacterial sinusitis in children is treated with one or two of the following antibiotics.
• Amoxicillin Amoxicillin;
• Amoxicillin/clavulamic acid augmentin;
• Erythromycin/sulfioxazole;
• Sulfamethoxazole/trimethoprim;
• Cefaclor; • Cefuroxime axetil;
• Cefprozil, • Cefpodoxime proxetil,
• Loracarbef;
• Clarithromycin;
• Clindamycin;
• It is common to choose one of the other antibiotics and treat it for 2-6 weeks.
• If you have a high fever and acute sinusitis, you should be hospitalized and treated with intravenous antibiotics.
• Sometimes treated with antibiotics and nasal corticosteroid sprays.
• Treatment with 5 drops of physiological saline in the left and right nasal passages 4 times a day for 10 days is said to have a good therapeutic effect. Of course, if necessary, surgical treatment is also performed.
2012 American Society of Infectious Diseases guidelines for the treatment of acute sinusitis in adults If you have the following symptoms or conditions 1 to 5, diagnose bacterial sinusitis rather than viral rhinosinusitis.
• Symptoms persist for at least 10 days and
• Does not recover with symptomatic treatment • Symptoms are severe, high fever, purulent runny nose, and face pain persist for 3 to 4 days.
• Respiratory infections that get worse and worse after they start • When symptoms get worse 5 to 6 days after the onset of respiratory symptoms
Bacterial rhinosinusitis is treated as follows.
• Amoxicillin/clavulamic acid;
• Doxycycline
• Cefpodoxime proxetil,
• Cefixime
• Treat with one of the following antibiotics. REFERENCE AND SOURCE: HARVARD MEDICAL SCHOOL, INFECTIOUS DISEASES IN PRIMARY CARE OCTOBER 14-16, 2015
Picture 112. Sinus X-ray.
• a-frontal sinus, b-ethmoid sinus, c-maxillary sinus. • Copyright ⓒ 2011 John Sangwon Lee, M.D., FAAP
Picture 113. X-ray of the sinuses.
• a-frontal sinus, b-ethmoid sinus, c-maxillary sinus. Copyright ⓒ 2011 John Sangwon Lee, M.D. FAAP
The following is an example of an Internet pediatric health consultation Q&A on “recurring allergic rhinitis and sinusitis”.
Q&A. allergic rhinitis sinusitis recurrence
Q.
• In the article below, I am a mother of a 6-year-old who inquired about my child’s headache several times.
• When the child wakes up at dawn or in the morning for 5 days, she said that she had a headache, so the pediatrics and adolescents took the pulse and the ophthalmologist took the intraocular pressure, but everything came out normal.
• Then, when her child woke up, one of her nostrils was blocked and the inside of her nose was swollen.
• So the pediatrician was on vacation, so she went to the otolaryngologist, and in the meantime, sinusitis.
• She has been taking the antibiotic Augmentin Duo and the steroid synthisone for coughing while she is on medication at the pediatrics department, and she had a headache while taking it.
• But when she took the medicine, her head didn’t hurt, and after 3 days after taking the medicine, her nose was strange, and when she went, she said that her nose was full of yellow noses, which is called sinusitis. How can you have a relapse so quickly?
• If you catch a cold while taking medicine, will it immediately recur?
• During that time, my nose was clean for about 3 weeks. She was treated for sinusitis for 3 months and 1 week, and after about 3 days she had sinusitis, it was amazing that she had sinusitis again.
• And she says the otolaryngologist thinks the child has sinusitis because of a drug called Zadi Ten. It’s because the medicine is holding the nose so tightly that it can’t be expelled.
• My child took the sinusitis medication and was taking only the preventive medicine called Zaditen twice a day.
• I follow the instructions of the pediatrician and pediatrician, but she only goes to the Lee Bin gynecology department. Johnny’s overall health is unstable.. What should I do? Besides, the medicines given to her by the Department of Ophthalmology are sulfa drugs, lulide suspension tablets for children, and a nasal decongestant, Shu…. (I can’t remember the name).
• I was wondering if it would work because I’ve taken all the drugs before. What would you like to do? Pediatrician Teacher Should I go back to the Pediatrics Department after the vacation is over?
A.
• Soon-hee
• Good morning. Thanks again for asking a good question. Thank you for providing detailed information such as the child’s age, gender, past medical history, and examination findings. I can understand to some extent my mother who is worried about me.
• In the meantime, the doctor has personally examined, diagnosed, and treated, so I’m worried about whether I can give any help.
• If I am a regular adolescent and doctor who treats my son, I think I can try the following treatment.
• As I said before, I think your child has atopic constitution.
• Most of the children with atopic constitution
• allergic rhinitis;
Sinusitis (sinusitis);
• Krupp, • bronchial asthma;
• atopic dermatitis;
• allergic conjunctivitis;
• headache,
• dizziness;
• Pseudoanemia;
• Allergy Shiner,
• milk allergy;
• Tension Fatigue Syndrome;
• Insect allergy, etc.
• There are several types of allergic conditions that can cause symptomatic symptoms.
• In fact, most of the people who suffer from these allergic diseases without realizing it, live without even knowing they have such allergies.
• I, too, was one of those people who struggled with this problem a lot before coming to the United States to study medicine.
• Unfortunately, there is no cure for allergies. The focus should be on prophylactic treatment. • Don’t worry, if you take preventative treatment and treat it well from time to time, you will not have such a big health problem.
• These days, there are many kinds of drugs for preventive treatment of such allergic diseases, and the side effects are few and the preventive treatment is good.
• First of all, I would like to point out that there are many causes of sinusitis. • It can recur unpredictably.
• Although it is common for school-aged children to get eight colds per year,
• The same study found that some children get it 22 times a year.
• In case of a cold, it is common for the virus that caused the cold to infect the nasal mucosa and pharyngeal mucosa and cause infectious diseases to the mucous membranes in the sinuses.
• As long as a secondary bacterial infection does not occur at this time, the common cold will heal naturally and the viral sinusitis may heal naturally.
• If you have a secondary bacterial (bacterial) infection in viral sinusitis caused by a cold, you have bacterial sinusitis.
• At this time, symptoms are more severe than those of a cold alone, and the runny nose is thicker, yellower, and sometimes bluish.
• Headache, fatigue, fever, and tenderness in the affected area of the sinuses.
• However, in some cases there may be few signs of such symptoms.
• As you know, the diagnosis of sinusitis is often made by referring to the symptomatic signs and past and present medical history, so doctors may sometimes misdiagnose it.
• In general, a presumptive diagnosis based on clinical experience without a sinus x-ray, CT scan, or MRI scan, and no bacteriological examination, and treatment by it are more common.
• In most children with allergic rhinitis, even when they don’t have a cold, the mucous membranes in the nasal passages may swell as well as the mucous membranes in the sinuses.
• Occasionally, a bacterial, virus, or fungal infection in the sinuses can cause sinusitis.
• Depending on which bacteria is causing the sinusitis, the age of your child with the sinus infection, the presence of allergic rhinitis, acute or chronic sinusitis, or other conditions have very different symptoms, severity, and treatment prognosis for sinusitis.
• If sinusitis occurs frequently, sometimes it is necessary to find out whether the immune function is normal or abnormal, and whether the ciliary function of the nasal and upper respiratory tract mucosal layers is normal.
• Keeping this complex medical knowledge in mind, sinusitis (sinusitis) does not get better even with proper treatment with antibiotics and other drugs, so there are times when sinusitis needs to be treated with surgery.
• Treatment with antibiotics usually lasts 10-14 days, sometimes as long as 6 weeks. • Even with such treatment, it may recur. Recurrence may occur even if prophylactic treatment is well taken to prevent recurrence.
• If it seems that children are suffering from sinusitis, as described above, since the causes of sinusitis are related to allergies, immune function, airway ciliary function, growth and development, etc., it is ideal to first receive diagnosis and treatment from the Department of Pediatrics.
• However, in some cases, of course, you may be treated by a specialist other than pediatricians, especially an otolaryngologist.
• For untreated sinusitis, several specialized specialists, such as an otolaryngologist, pediatric allergy and immunologist, pediatric infectious disease specialist, and pediatric respiratory specialist, are sometimes referred to each other for team treatment.
• When receiving such treatment, if possible, depending on the judgment of a regular pediatrician, refer to an appropriate otolaryngologist or other special specialist, and the treatment as a team of specialists will be the most ideal treatment method.
• When treating in this way, because each specialist listens to each other’s opinions and treats them in the most appropriate way, regular pediatricians and other specialists can treat with almost the same drugs.
• However, when treatment is performed in this way, medical expenses are high, and social medical administration conditions for such treatment must be established.
• In general, when treating acute sinusitis, a runny nose specimen obtained from the nasal passages is selected and treated with antibiotics based on information obtained from clinical experience without Gram-stained bacterial microscopy and bacteriological examination, but sometimes sinusitis with systemic symptoms; In particular, when suffering from severe bacterial sinusitis or incurable sinusitis, a bacteriological test can be performed with a specimen obtained from the mucous membrane of the nasal cavity or a specimen obtained by needle puncture from a sinus with sinusitis.
• In general, it’s not worthwhile to do a routine bacteriological test to see what type of bacteria is causing sinusitis.
• Sometimes it is ideal to treat sinusitis with the most appropriate antibiotic by doing such a bacteriological test to find out which bacteria is causing the sinusitis and also for susceptibility to antibacterial agents that can treat sinusitis infected with that bacteria.
• Without bacteriological testing, the sulfa drugs Septra or Augmentin, etc., and antihistamines or nasal mucosal decongestants can constrict the nasal mucosal capillaries and treat sinusitis.
• In addition, it is sometimes necessary to check whether white blood cell function, upper respiratory tract mucosa function, and immune function are normal.
• If you have allergic rhinitis, sinusitis, or bronchial asthma, manage your environment to avoid exposure to foods that can cause allergic diseases such as milk, environmental pollution, house dust mites, stress, pets, drugs, smoking, etc. It is also very important to prevent allergies by taking good care of it, and treatment and prevention with second-generation antihistamines such as Claritin-Loratadine, or Cromolyn sodium nasal spray, or corticosteroid nasal analgesics, etc. It can be treated with antibiotics.
• For such treatment, as mentioned before, it is appropriate to receive treatment from a regular pediatrician, and if necessary, you can refer to a pediatric allergist or an otolaryngologist for treatment together.
• I am telling you that this treatment method can be treated as such.
• When administering diagnostic treatment, it is important to choose the form of the drug based on the judgment of your child’s doctor (if your child is mature).
• You should discuss with your doctor the type, dosage, and duration of your medication.
• www.dsrleepediatrics.com- Volume 15 Children and adolescents If you read a lot of allergies and autoimmune diseases, you will find a lot of information and answers about your questions there. In particular, please read a lot about sinusitis, asthma, allergic rhinitis, allergens, antigens, etc.
• I would like to reiterate that parents must take the primary responsibility and actively participate in the effective treatment of allergic diseases.
• If the problem persists, please continue to see a pediatrician and discuss the problem. Please visit again if you have more questions. Thank you. Lee Sang-won .MD
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy of Pediatrics
- www.drleepediatrics.com 제 6권 신생아 성장 발육 육아 질병
-
www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th — 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
-
Childhood Emergencies in the Office, Hospital and Community, American Academy of Pediatrics
-
Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
-
Emergency care, harvey grant and robert murray
-
Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
-
Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
-
Immediate care of the acutely ill and injured, Hugh E. Stephenson, Jr
-
The Critically Ill Child, Diagnosis and Management, Edited by Clement A. Smith
-
Emergency Medical Services for Children: The Role of the Primary Care Provider, America Academy of Pediatrics
-
Quick Reference To Pediatric Emergencies , Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
-
Manual of Emergency Care
-
응급환자관리 정담미디어
-
소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
-
Neonatal Resuscitation American heart Association
-
Neonatology Jeffrey J.Pomerance, C. Joan Richardson
-
Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A. Gershon, Catherine Wilfert
-
The Harriet Lane Handbook 19th Edition
-
소아과학 대한교과서
-
제1권 소아청소년 응급의료 참조문헌과 출처
-
Other
- Copyright ⓒ 2015 John Sangwon Lee, MD., FAAP
- “부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
- “The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances. “Parental education is the best medicine.”